

Computed Tomography in Infectious Endocarditis
- PMID: 39131217
- PMCID: PMC11308100
- DOI: 10.1016/j.jscai.2023.101292
Computed Tomography in Infectious Endocarditis
Abstract
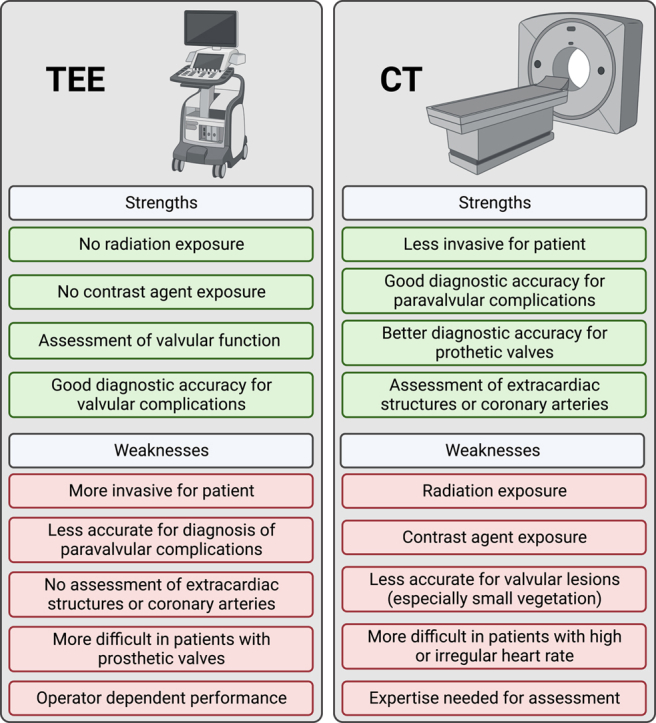
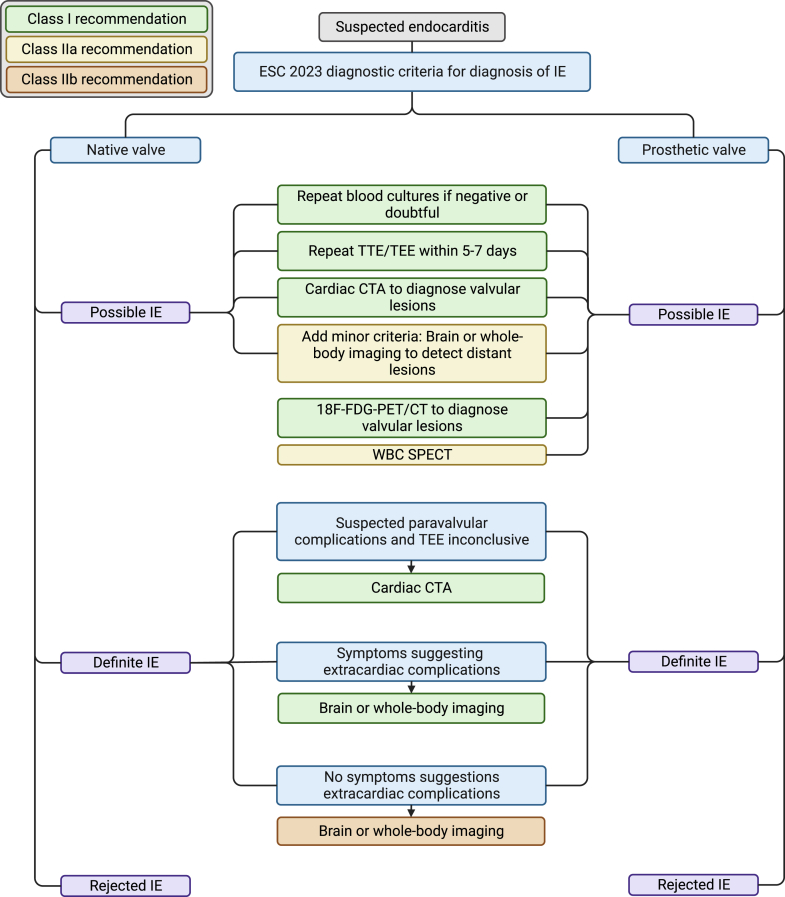
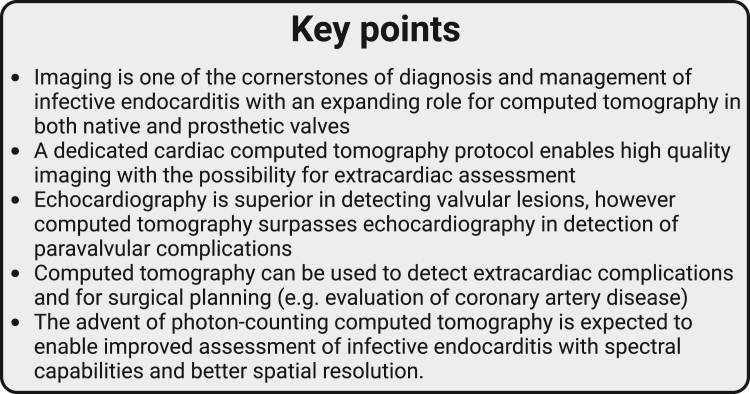
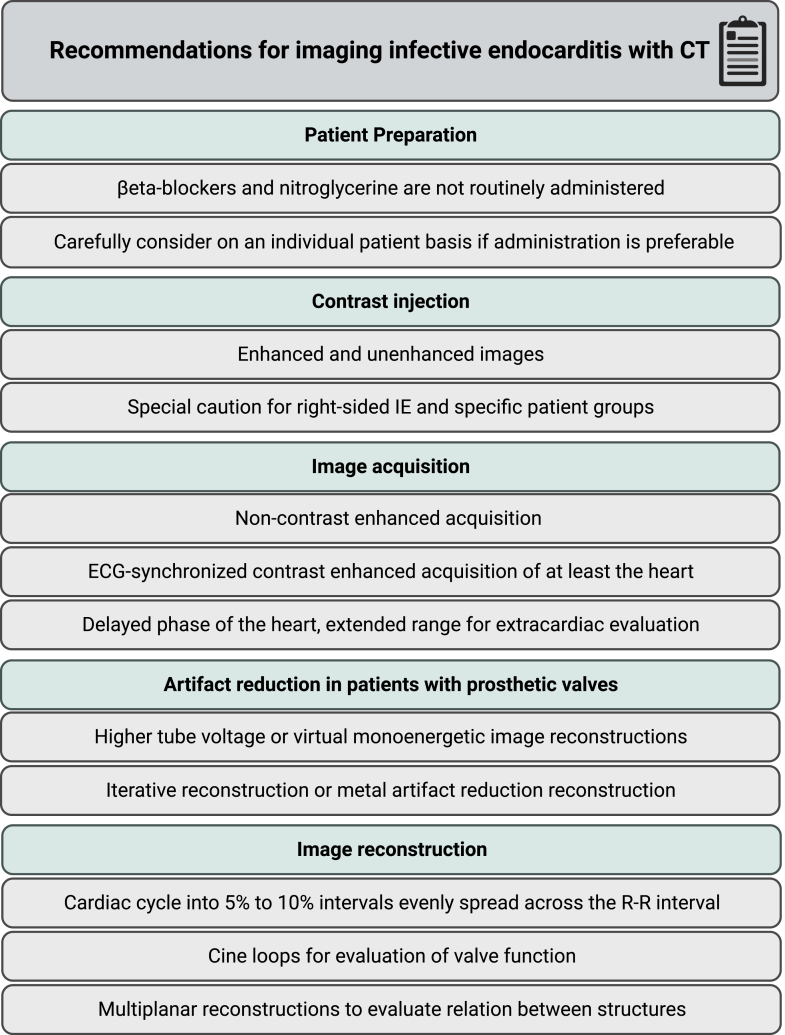
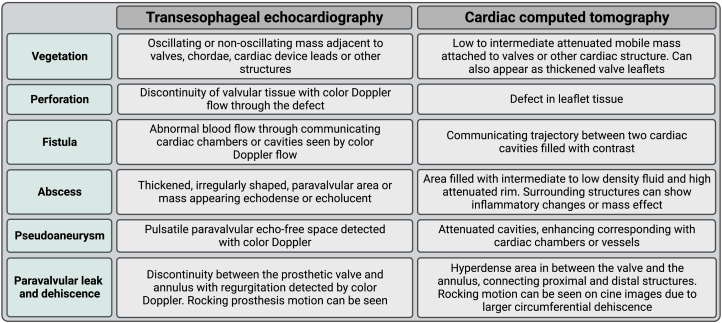
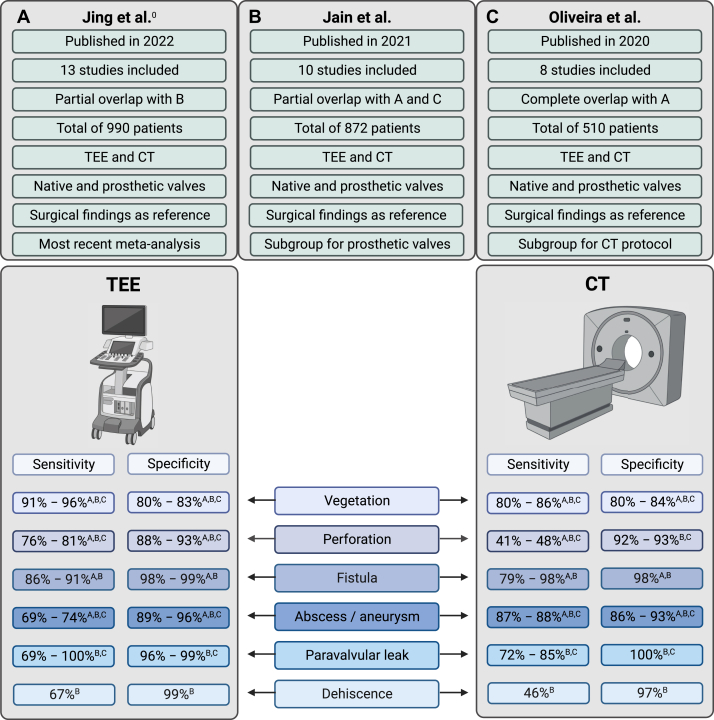
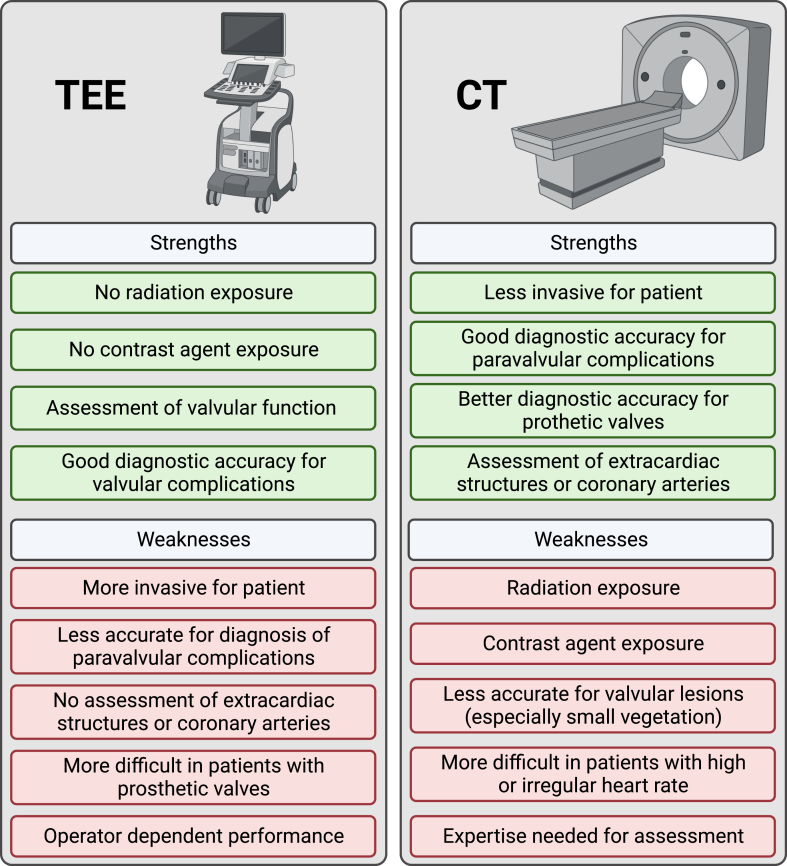
Imaging is one of the cornerstones in diagnosis and management of infective endocarditis, underlined by recent guidelines. Echocardiography is the first-line imaging technique, however, computed tomography (CT) has a class I recommendation in native and prosthetic valve endocarditis to detect valvular lesions in case of possible endocarditis and to detect paravalvular and periprosthetic complications in case of inconclusive echocardiography. Echocardiography has a higher diagnostic accuracy than CT in detecting valvular lesions, but not for diagnosing paravalvular lesions where CT is superior. Additionally, CT is useful and recommended by guidelines to detect extracardiac manifestations of endocarditis and in planning surgical treatment including assessment of the coronary arteries. The advent of photon-counting CT and its improved spatial resolution and spectral imaging is expected to expand the role of CT in the diagnosis of infective endocarditis. In this review, we provide an overview of the current role of CT in infective endocarditis focusing on image acquisition, image reconstruction, interpretation, and diagnostic accuracy.
Keywords: cardiac imaging; computed tomography; infective endocarditis.
© 2023 The Author(s).
Figures

References
-
- Writing Committee Members. Otto C.M., Nishimura R.A., et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2021;77(4):e25–e197. doi: 10.1016/j.jacc.2020.11.018. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
