

Clinical Characteristics, Outcomes, and Epidemiological Trends of Patients Admitted With Type 2 Myocardial Infarction
- PMID: 39131460
- PMCID: PMC11307827
- DOI: 10.1016/j.jscai.2022.100395
Clinical Characteristics, Outcomes, and Epidemiological Trends of Patients Admitted With Type 2 Myocardial Infarction
Abstract
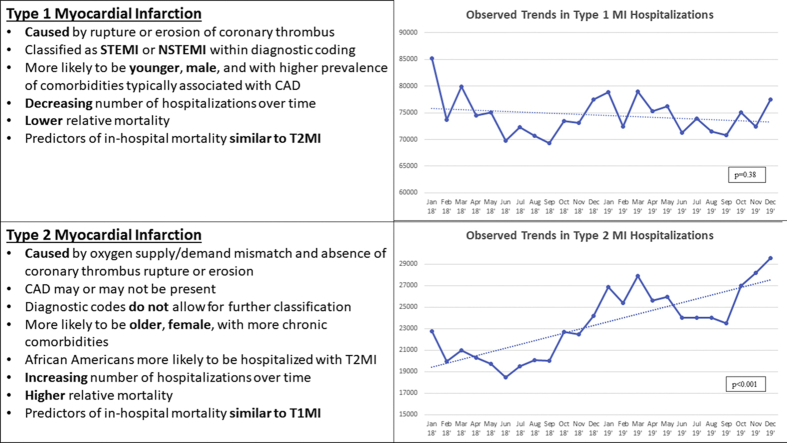
Background: Type 2 myocardial infarction (T2MI) was first established as a unique entity in 2007. However, its clinical features are not well characterized. This study aimed to determine the clinical characteristics, predictors of mortality, and hospitalization trends of patients with T2MI.
Methods: The National Inpatient Sample database was queried for patients hospitalized in the United States with T2MI (January 2018 to December 2019). Data were used to assess baseline characteristics, primary diagnoses, predictors of mortality, and hospitalization and mortality trends of T2MI.
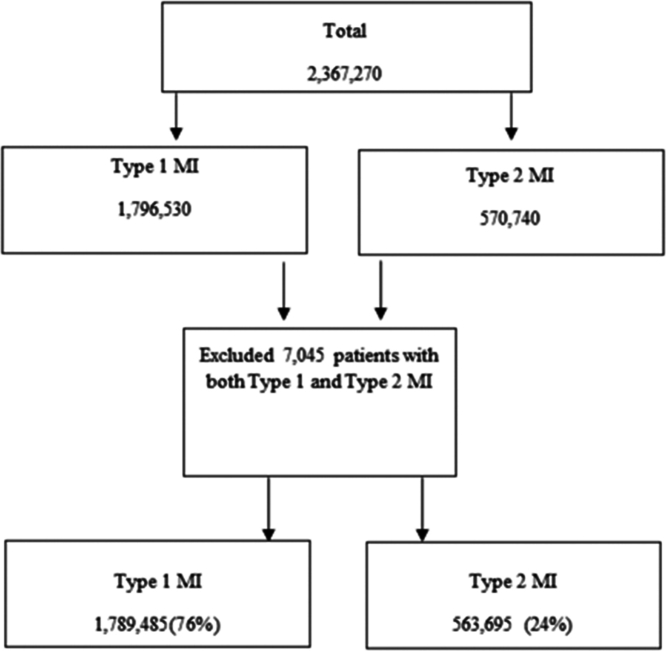
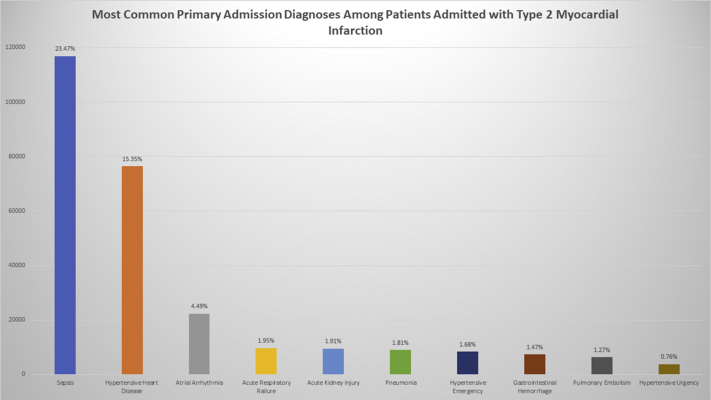
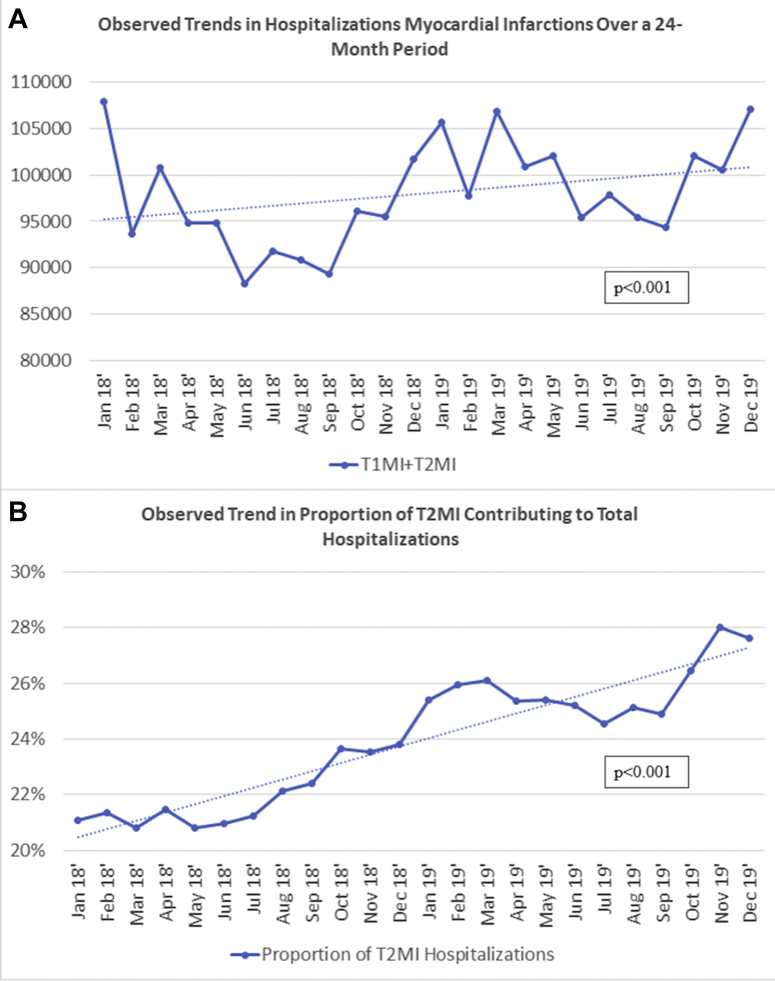
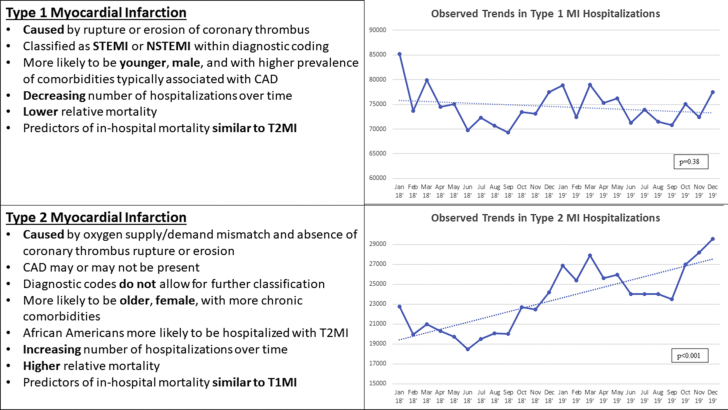
Results: During the 24-month study period, 1,789,485 (76%) patients were admitted with type 1 myocardial infarction (T1MI) and 563,695 (24%) were admitted with T2MI. Patients with T2MI were more likely to be older (71 vs 68 years; P < .001) and female (47.5% vs 38.3%; P < .001), with fewer comorbidities related to coronary atherosclerosis. African Americans were the only race with a significantly higher rate of hospitalization for T2MI (15.9% vs 11.6%; P < .001). The predictors of mortality were similar in both the T2MI and T1MI cohorts. Sepsis (23.47%), hypertensive heart disease (15.35%), and atrial arrhythmias (4.49%) were the most common principal diagnoses for T2MI. T2MI hospitalizations trended consistently upward during the study period. Monthly in-hospital mortality rates were consistently higher for T2MI versus T1MI (P < .001).
Conclusions: T2MI is a unique and heterogeneous clinical entity. Despite increased awareness, there is a lack of standardization of medical management and timing for revascularization, even as mortality rates remain persistently elevated compared with T1MI. Certain demographics, including African Americans, may be disproportionately affected.
Keywords: National Inpatient Sample; mortality; outcomes; type 2 myocardial infarction.
© 2022 The Authors.
Figures

References
-
- Thygesen K., Alpert J.S., White H.D., et al. Universal definition of myocardial infarction. Circulation. 2007;116(22):2634–2653. - PubMed
-
- Cediel G., Gonzalez-Del-Hoyo M., Carrasquer A., Sanchez R., Boqué C., Bardají A. Outcomes with type 2 myocardial infarction compared with non-ischaemic myocardial injury. Heart. 2017;103(8):616–622. - PubMed
-
- McCarthy C.P., Kolte D., Kennedy K.F., Vaduganathan M., Wasfy J.H., Januzzi J.L. Patient characteristics and clinical outcomes of type 1 versus type 2 myocardial infarction. J Am Coll Cardiol. 2021;77(7):848–857. - PubMed
LinkOut - more resources
Full Text Sources
