

Management of Pediatric Pulmonary Vein Stenosis
- PMID: 39131478
- PMCID: PMC11307749
- DOI: 10.1016/j.jscai.2022.100391
Management of Pediatric Pulmonary Vein Stenosis
Abstract
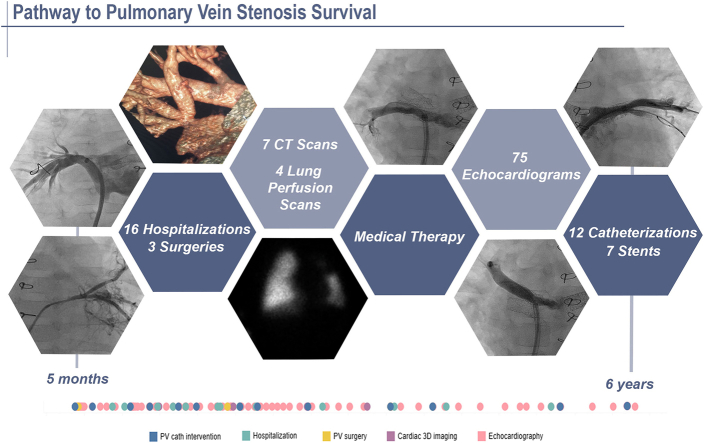
Pediatric intraluminal pulmonary vein stenosis has evolved into a chronic illness, with improving survival. Although significant knowledge gaps remain, medical providers have found success in the management of patients with pulmonary vein stenosis using a comprehensive multimodality treatment strategy. This review discusses the core principles employed by 4 centers dedicated to improving pulmonary vein stenosis outcomes, including how to make the diagnosis, educating the family, treatment strategy, the importance of surveillance, and the management of symptoms and comorbidities.
Keywords: congenital heart disease; management; pulmonary vein stenosis; therapy.
© 2022 The Author(s).
Figures







References
Publication types
LinkOut - more resources
Full Text Sources
