

Interventional Cardiac Procedures and Pregnancy
- PMID: 39131483
- PMCID: PMC11307807
- DOI: 10.1016/j.jscai.2022.100427
Interventional Cardiac Procedures and Pregnancy
Abstract
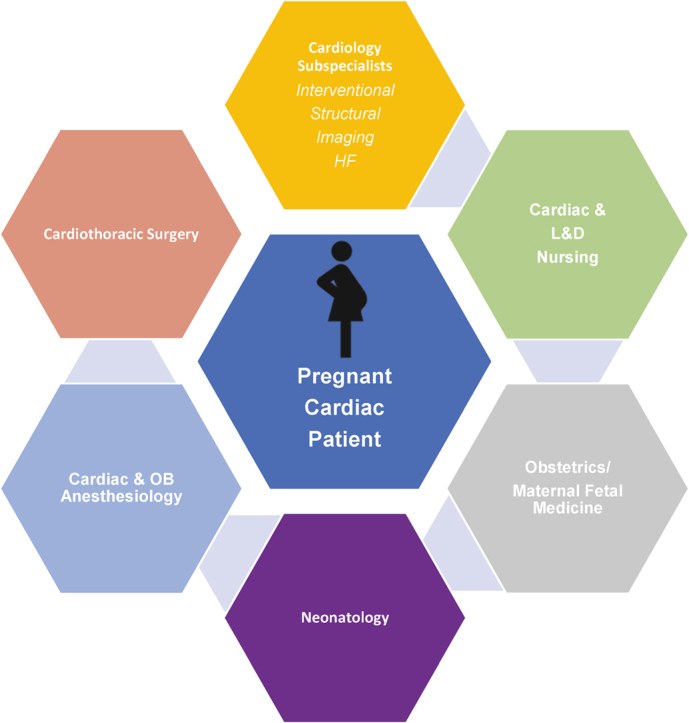
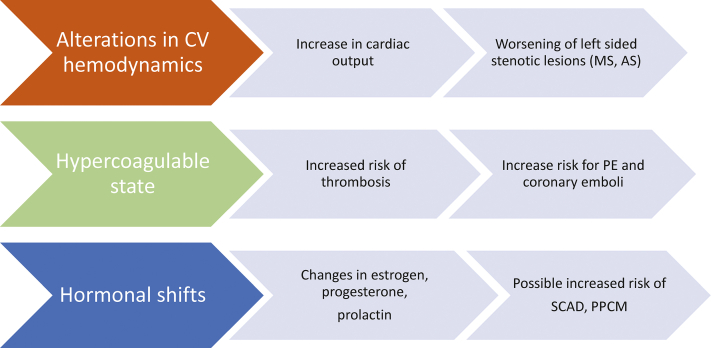
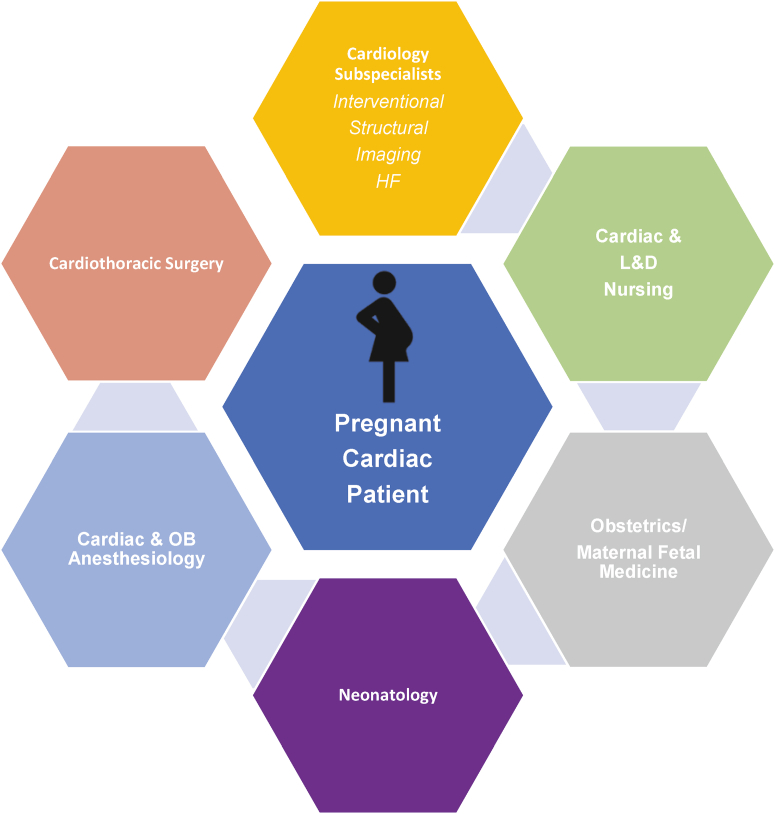
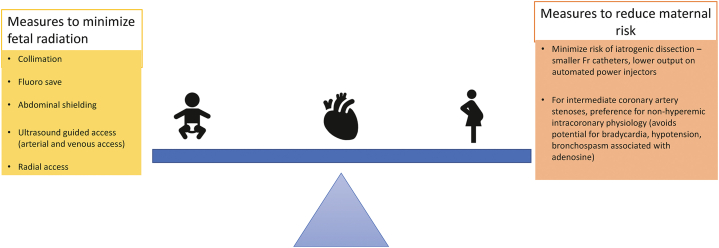
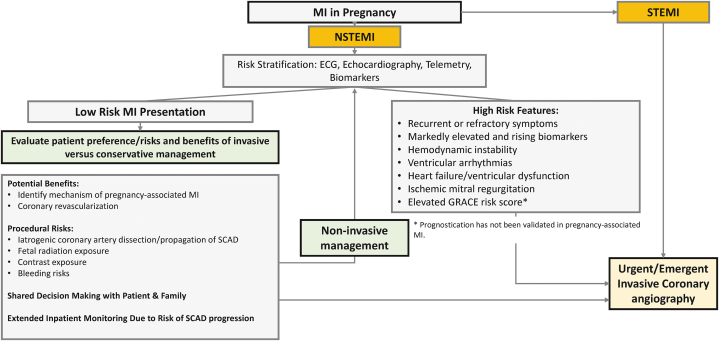
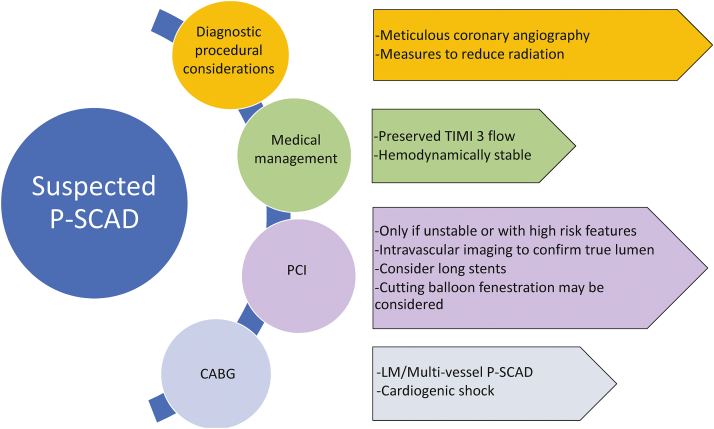
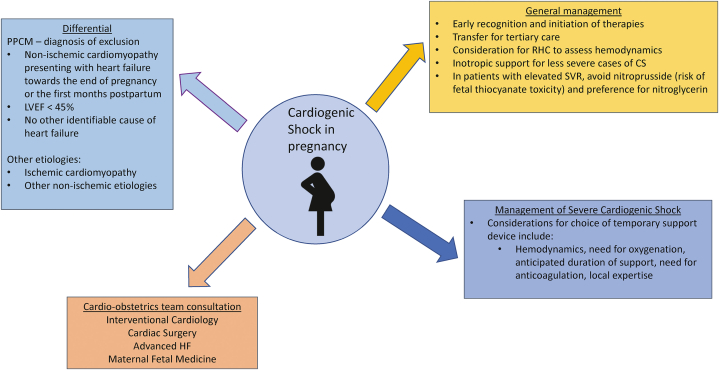
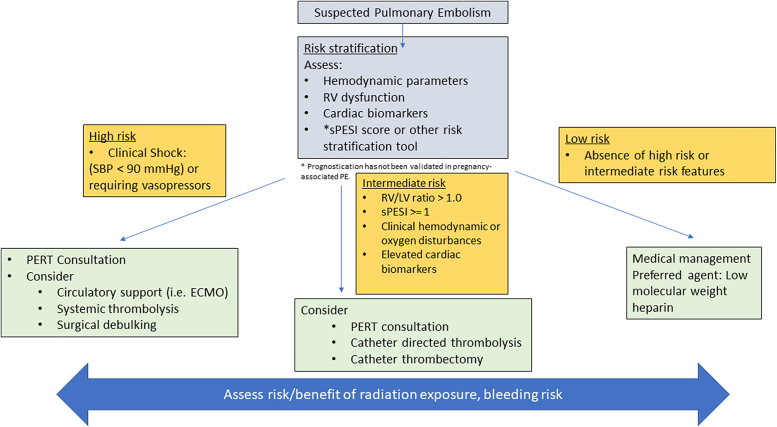
As the average maternal age advances with increasing concurrent cardiovascular disease risk factors, more women are entering pregnancy with or at risk for various cardiovascular conditions. Although rare, pregnant patients may require various cardiac interventions in the catheterization laboratory. An understanding of indications for intervention in pregnant patients with conditions such as myocardial infarction, severe valvular disease, and cardiogenic shock is critical to optimizing both fetal and maternal outcomes. This document highlights the most common cardiovascular conditions that may be encountered during pregnancy that may require intervention and highlights indications for intervention and periprocedural considerations to facilitate favorable maternal and fetal outcomes.
Keywords: cardiogenic shock; maternal-fetal medicine; myocardial infarction; percutaneous coronary intervention; peripartum cardiomyopathy; pregnancy-associated spontaneous coronary artery dissection.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
