

One-Year Clinical Outcomes Following Mechanical Thrombectomy for Deep Vein Thrombosis: A CLOUT Registry Analysis
- PMID: 39131784
- PMCID: PMC11308810
- DOI: 10.1016/j.jscai.2024.101307
One-Year Clinical Outcomes Following Mechanical Thrombectomy for Deep Vein Thrombosis: A CLOUT Registry Analysis
Abstract
Background: Mechanical thrombectomy is a promising treatment option for deep vein thrombosis; however, long-term data are lacking. Here, we report for the first time the 1-year clinical outcomes from the completely enrolled ClotTriever Outcomes (CLOUT) registry evaluating mechanical thrombectomy with the ClotTriever System (Inari Medical).
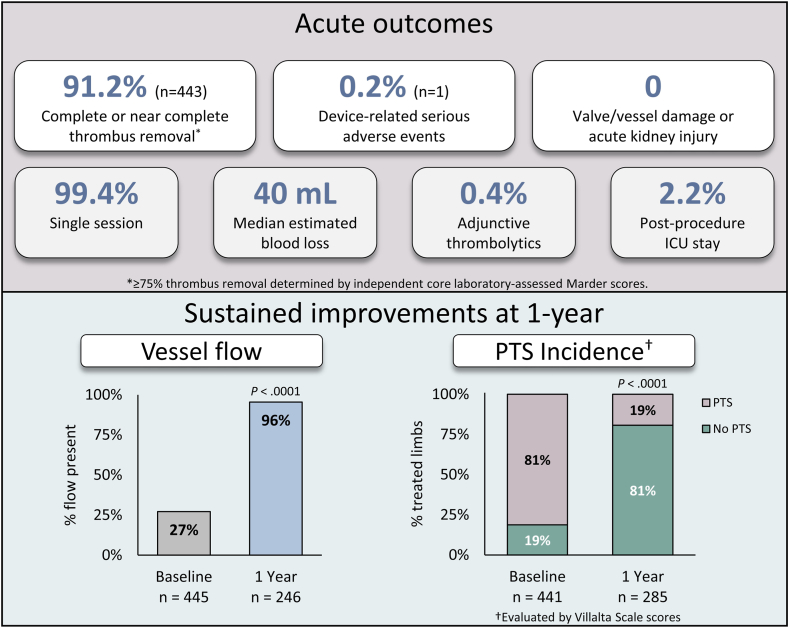
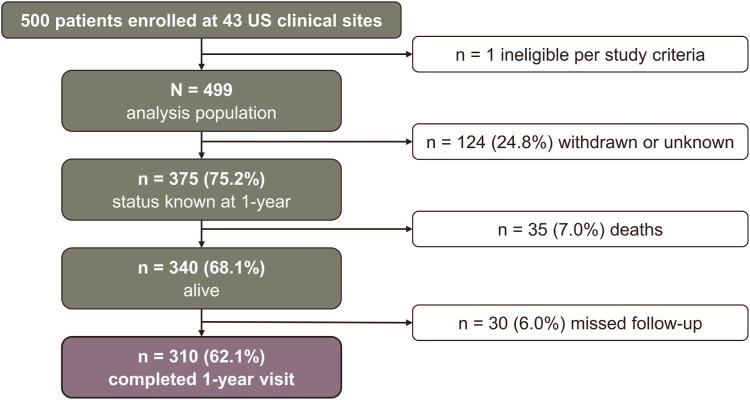
Methods: The CLOUT registry (NCT03575364) is a prospective, multicenter, single-arm study that enrolled 500 patients with proximal lower extremity deep vein thrombosis. Prespecified 1-year outcomes include Villalta score and corresponding postthrombotic syndrome (PTS) severity, duplex ultrasound findings of patency (defined as the presence of flow with normal or partial compressibility), Revised Venous Clinical Severity Score, and quality of life (QoL).
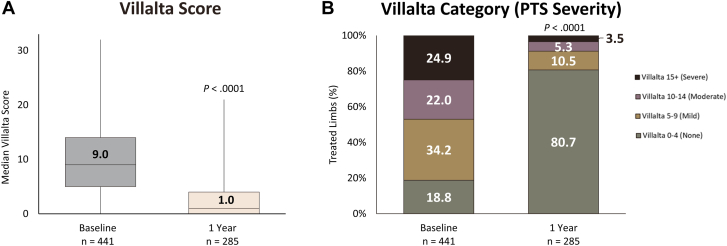
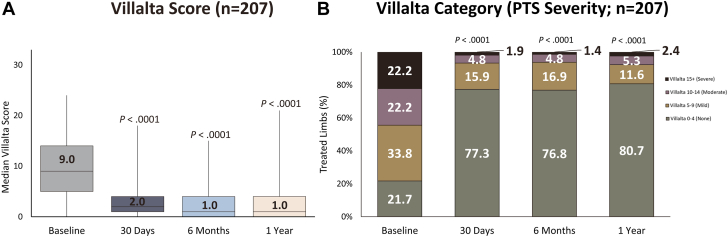
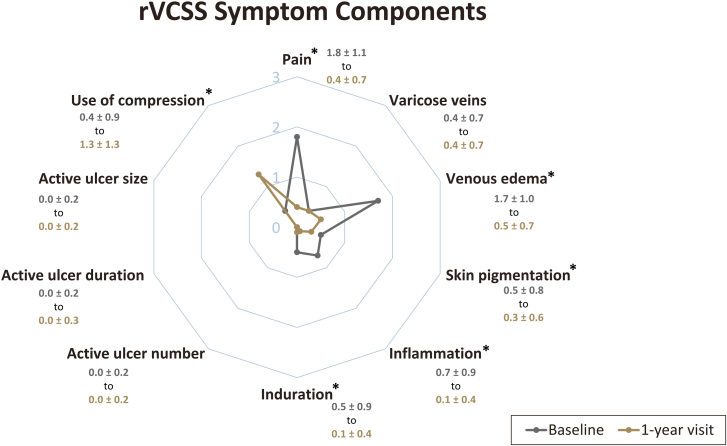
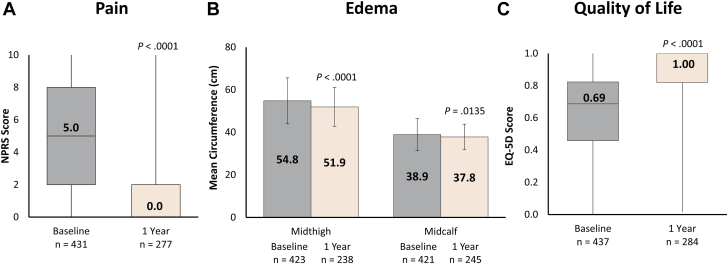
Results: In CLOUT, the median age was 61.9 years and 50.5% of patients were women. A total of 310 patients completed the 1-year visit. The 1-year PTS rate (Villalta score ≥ 5) was 19.3% and the moderate-to-severe PTS rate (Villalta score ≥ 10) was 8.8%. Median Villalta score decreased from 9.0 (IQR, 5.0-14.0) at baseline to 1.0 (IQR, 0.0-4.0) at 1 year (P < .0001). Similar rates of PTS and moderate-to-severe PTS were observed among limbs assessed at all study time points. Patency was observed in 94.2% of limbs. Median Revised Venous Clinical Severity Score was 6.0 (IQR, 3.0-9.0) at baseline and 3.0 (IQR, 1.0-4.0) at 1 year (P < .0001). Additionally, 90.4% of patients experienced improvements in QoL.
Conclusions: One-year outcomes from the CLOUT registry demonstrate low PTS rates and preserved patency accompanied by improved symptom relief and QoL. Study follow-up through 2 years is ongoing.
Keywords: deep vein thrombosis; intervention; lower extremity; mechanical thrombectomy; postthrombotic syndrome; prospective studies; quality of life.
© 2024 The Author(s).
Figures
References
-
- Jaff M.R., McMurtry M.S., Archer S.L., et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123(16):1788–1830. doi: 10.1161/CIR.0b013e318214914f. - DOI - PubMed
-
- Mazzolai L., Aboyans V., Ageno W., et al. Diagnosis and management of acute deep vein thrombosis: a joint consensus document from the European Society of Cardiology working groups of aorta and peripheral vascular diseases and pulmonary circulation and right ventricular function. Eur Heart J. 2018;39(47):4208–4218. doi: 10.1093/eurheartj/ehx003. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
