Outcomes of Transcatheter Aortic Valve Replacement Using Third-Generation Balloon-Expandable Versus Self-Expanding Valves: A Meta-analysis
- PMID: 39131997
- PMCID: PMC11308705
- DOI: 10.1016/j.jscai.2024.102146
Outcomes of Transcatheter Aortic Valve Replacement Using Third-Generation Balloon-Expandable Versus Self-Expanding Valves: A Meta-analysis
Abstract
Background: The choice of transcatheter aortic valve replacement (TAVR) prosthesis is crucial in optimizing short- and long-term outcomes. The objective of this study was to conduct a meta-analysis comparing outcomes of third-generation balloon-expandable valves (BEV) vs self-expanding valves (SEV).
Methods: Electronic databases were searched from inception to June 2023 for studies comparing third-generation BEV vs SEV. Primary outcome was all-cause mortality. Secondary outcomes included clinical and hemodynamic end points. Random-effects models were used to calculate pooled odds ratios (ORs) or weighted mean differences (WMDs).
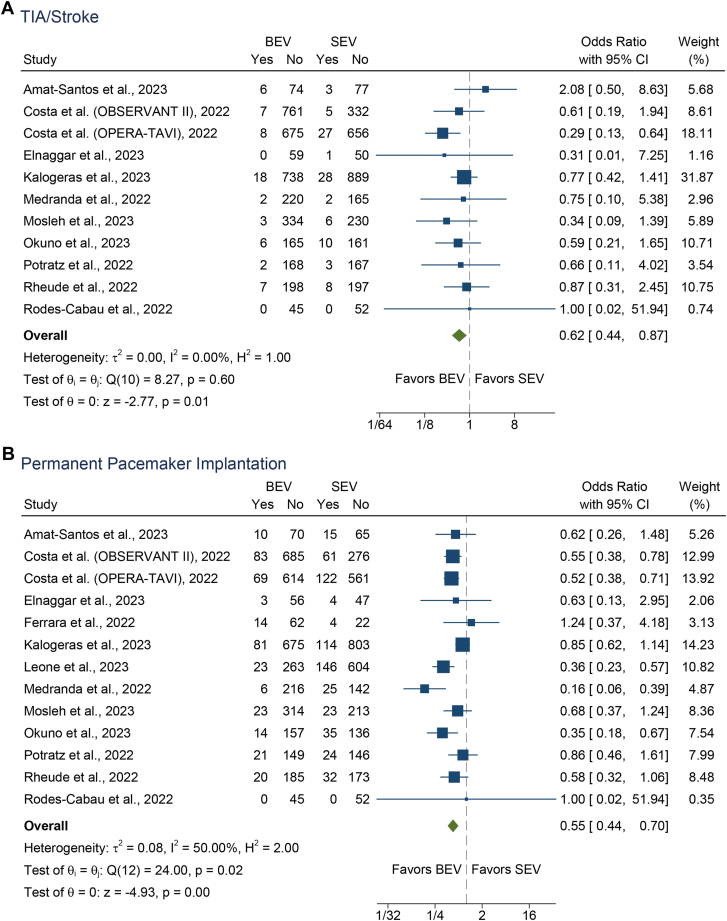
Results: The meta-analysis included 16 studies and 10,174 patients (BEV, 5753 and SEV, 4421). There were no significant differences in 1-year all-cause mortality (OR, 1.15; 95% CI, 0.89-1.48) between third-generation BEV vs SEV. TAVR with third generation BEV was associated with a significantly lower risk of TIA/stroke (OR, 0.62; 95% CI, 0.44-0.87), permanent pacemaker implantation (OR, 0.55; 95% CI, 0.44-0.70), and ≥moderate paravalvular leak (PVL, OR, 0.43; 95% CI, 0.25-0.75), and higher risk of ≥moderate patient-prosthesis mismatch (OR, 3.76; 95% CI, 2.33-6.05), higher mean gradient (WMD, 4.35; 95% CI, 3.63-5.08), and smaller effective orifice area (WMD, -0.30; 95% CI, -0.37 to -0.23), compared with SEV.
Conclusion: In this meta-analysis, TAVR with third-generation BEV vs SEV was associated with similar all-cause mortality, lower risk of TIA/stroke, permanent pacemaker implantation, and ≥moderate PVL, but higher risk of ≥moderate patient-prosthesis mismatch, higher mean gradient, and smaller effective orifice area. Large, adequately powered randomized trials are needed to evaluate long-term outcomes of TAVR with latest generations of BEV vs SEV.
Keywords: balloon-expandable valve; outcomes; self-expanding valve; transcatheter aortic valve replacement.
© 2024 The Author(s).
Figures