

Iatrogenic Aortocoronary Dissection During Right Coronary Artery Procedures: A Systematic Review of the Published Literature
- PMID: 39132357
- PMCID: PMC11308116
- DOI: 10.1016/j.jscai.2022.100443
Iatrogenic Aortocoronary Dissection During Right Coronary Artery Procedures: A Systematic Review of the Published Literature
Abstract
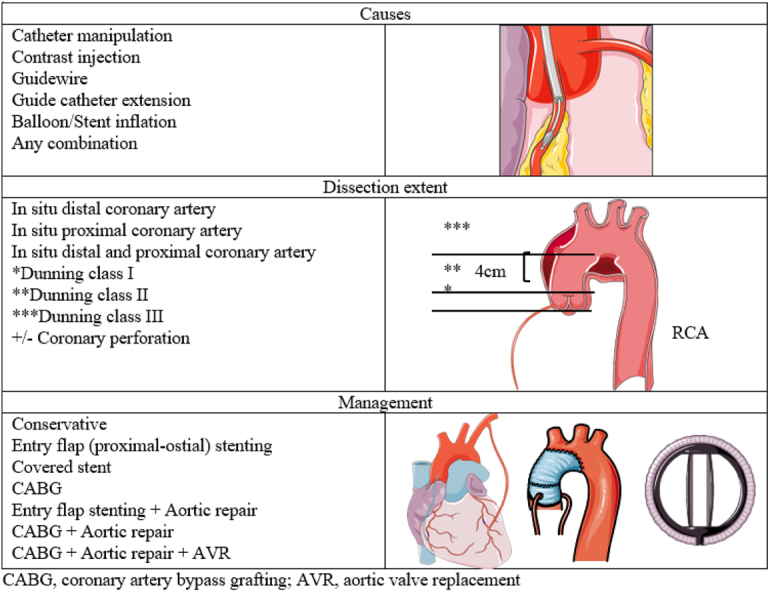
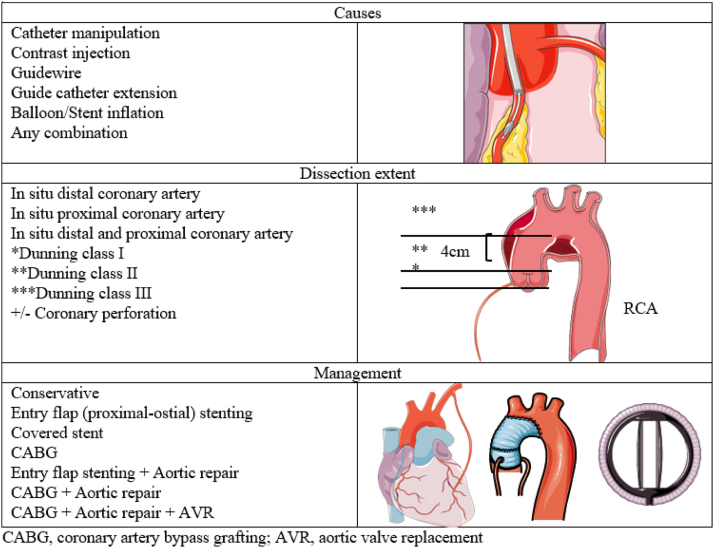
Iatrogenic aortocoronary dissection (IACD) occurs mainly during procedures involving the right coronary artery (RCA) and can result in disabilities, the need for urgent complex surgery, and even death. The risk factors for IACD are ill characterized, and the best management strategy is questionable; thus, there is a need to evaluate the characteristics, treatment options, and outcomes of patients with IACD of the RCA. We searched medical databases for publications on IACD of the RCA to present the characteristics of the procedures, management, and outcomes. We report 142 cases of IACD of the RCA, reported between 1973 and 2021. The mean age of the patients was 63.0 years, 81 (57%) were men, 75 (52.8%) presented with stable angina, and 29 (20.4%) had chronic total occlusion of the RCA. The most used catheter shapes were Judkins right (42%) and Amplatz left (25%), and most (56%) catheters were used during percutaneous coronary interventions. Guiding catheters were used in 38% (19/50) of diagnostic procedures when IACD occurred. A catheter size of ≤5F was used in only 3 cases. The catheter size was 6F in 22% of the cases, >6F in 23%, and not reported in 52%. A high-grade dissection (Dunning class III) occurred in 54% (77/142) of the cases. Stenting of the RCA ostium was performed in 88 (62%) of the cases, conservative treatment in 25 (18%), and surgery in 40 (28%) (aortic root repair [5%], coronary artery bypass grafting and aortic root repair [11%], and coronary artery bypass grafting alone [10%]). The mortality rate was 6.5% (5/77) among patients with class III dissection. Each patient should be considered independently. The most frequent intervention was to seal the dissection with a stent in the ostial RCA. However, in select cases published in the literature, a conservative approach was a feasible and successful option.
Keywords: aortocoronary dissection; catheter-induced aortic dissection; catheter-induced aortocoronary dissection; iatrogenic coronary dissection; stent.
© 2022 The Author(s).
Figures
References
-
- Pérez-Castellano N., García-Fernández M.A., García E.J., Delcán J.L. Dissection of the aortic sinus of Valsalva complicating coronary catheterization: cause, mechanism, evolution, and management. Cathet Cardiovasc Diagn. 1998;43(3):273–279. - PubMed
-
- Yip H.K., Wu C.J., Yeh K.H., et al. Unusual complication of retrograde dissection to the coronary sinus of Valsalva during percutaneous revascularization: a single-center experience and literature review. Chest. 2001;119(2):493–501. - PubMed
-
- Dunning D.W., Kahn J.K., Hawkins E.T., O’Neill W.W. Iatrogenic coronary artery dissections extending into and involving the aortic root. Catheter Cardiovasc Interv. 2000;51(4):387–393. - PubMed
-
- Moles V.P., Chappuis F., Simonet F., et al. Aortic dissection as complication of percutaneous transluminal coronary angioplasty. Cathet Cardiovasc Diagn. 1992;26(1):8–11. - PubMed
-
- Ahmed A.A.M., Mahadevan V.S., Webb S.W., MacGowan S.W. Glue aortoplasty repair of aortic dissection after coronary angioplasty. Ann Thorac Surg. 2001;72(3):922–924. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
