

Feasibility and Safety of Intracardiac Echocardiography Use in Transcatheter Left Atrial Appendage Closure Procedures
- PMID: 39132376
- PMCID: PMC11307399
- DOI: 10.1016/j.jscai.2022.100510
Feasibility and Safety of Intracardiac Echocardiography Use in Transcatheter Left Atrial Appendage Closure Procedures
Abstract
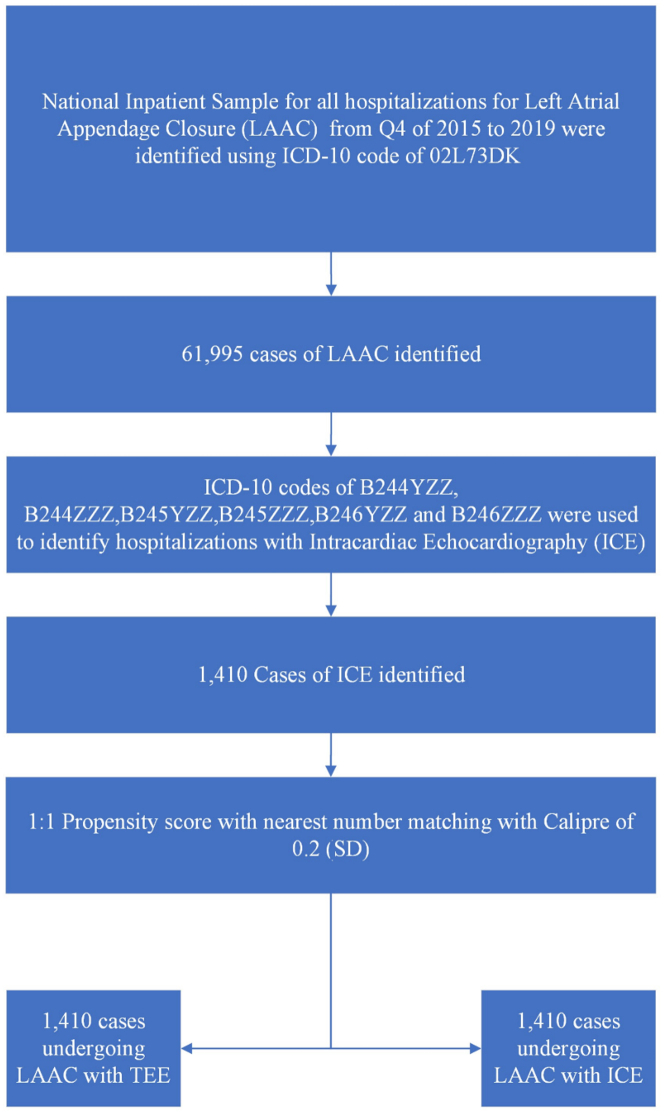
Background: Left atrial appendage closure (LAAC) is usually performed under the guidance of transesophageal echocardiography (TEE). Data on the safety of intracardiac echocardiogram (ICE)-guided LAAC from a real-world population in the United States remain limited. In this study, the aim was to evaluate the trends and outcomes of ICE-guided LAAC procedures using the US National Inpatient Sample.
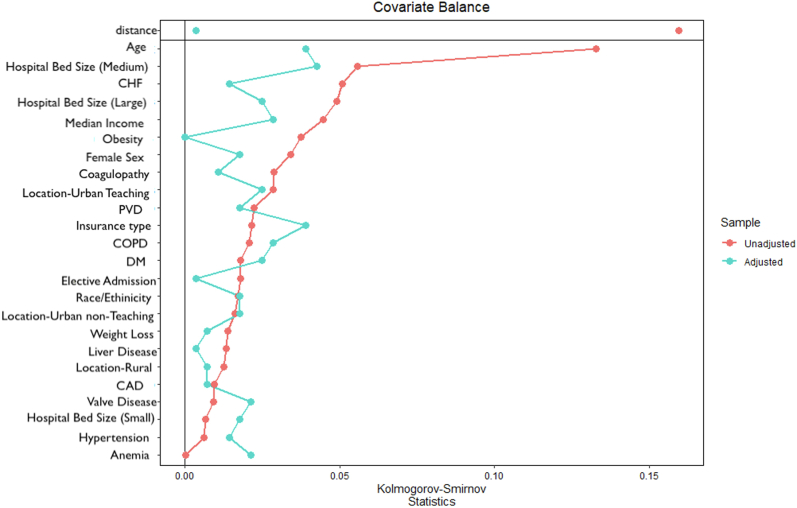
Methods: This study used the National Inpatient Sample database from quarter 4 of 2015 to 2019. We used a propensity-matched analysis and adjusted odds ratios for in-hospital outcomes/complications. A P value of <.05 was considered significant.
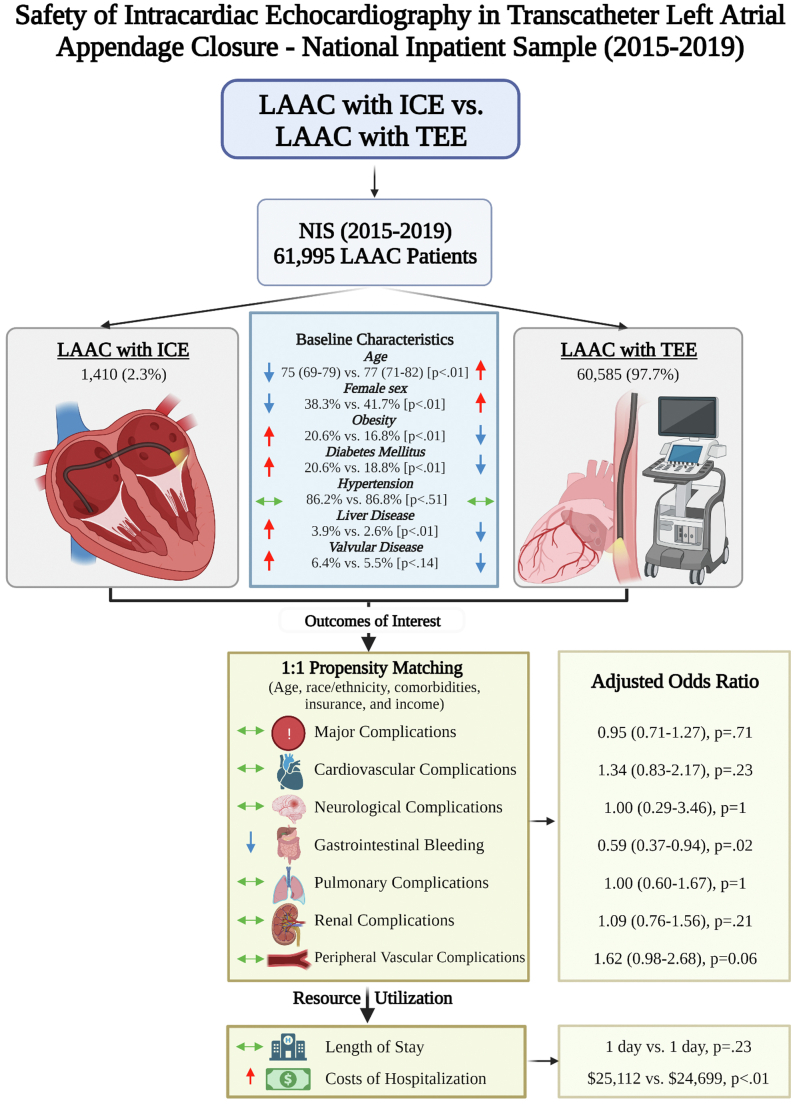
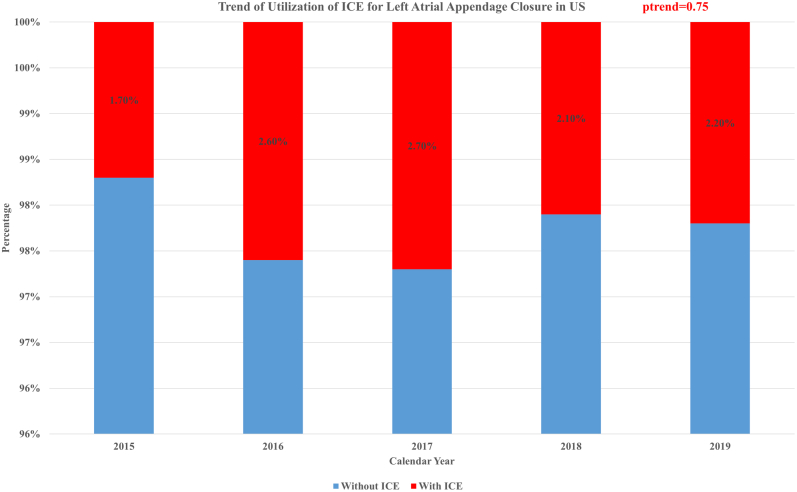
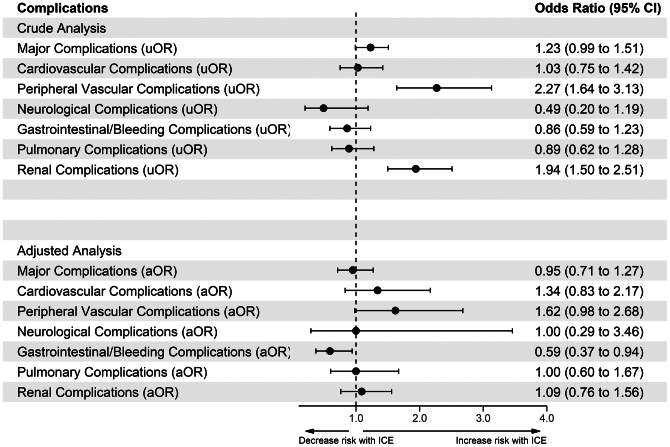
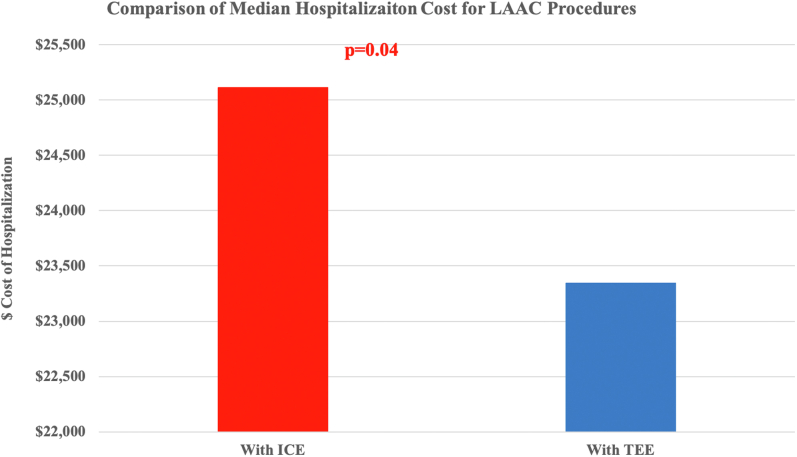
Results: We identified 61,995 weighted LAAC cases. Of these, 1410 patients had ICE-guided LAAC with a lower median age than the patients who had TEE-guided LAAC (75 vs 77 years; P ≤ .01). The use of ICE-guided LAAC increased from 1.7% in 2015 to 2.2% in 2019 (P trend = .75). Major, cardiovascular, neurologic, and pulmonary complications were similar for ICE-guided and TEE-guided LAAC on adjusted analysis. On propensity-matched analysis, the overall vascular complication rates were similar. However, retroperitoneal bleeding remained significantly higher (0.7% vs 0%) with ICE. Gastrointestinal bleeding complications were more frequent in TEE-guided LAAC (3.5% vs 2.1%). The length of stay was similar for both groups (median = 1 day; P = .23); however, ICE was associated with $1769 excess cost of hospitalization ($25,112 vs $23,343; P = .04).
Conclusions: ICE-guided LAAC is safer than TEE-guided LAAC, with similar rates of major complications. However, ICE use was associated with lower rates of gastrointestinal bleeding and higher rates of retroperitoneal bleeding. In addition, ICE-guided LAAC is associated with a similar length of stay but higher costs of hospitalization.
Keywords: echocardiography; intracardiac echocardiography; left atrial appendage closure.
© 2022 The Author(s).
Figures
References
-
- Holmes D.R.J., Kar S., Price M.J., et al. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial. J Am Coll Cardiol. 2014;64(1):1–12. doi: 10.1016/j.jacc.2014.04.029. - DOI - PubMed
LinkOut - more resources
Full Text Sources
