

The Intra-aortic Balloon Pump: A Focused Review of Physiology, Transport Logistics, Mechanics, and Complications
- PMID: 39132456
- PMCID: PMC11307388
- DOI: 10.1016/j.jscai.2024.101337
The Intra-aortic Balloon Pump: A Focused Review of Physiology, Transport Logistics, Mechanics, and Complications
Abstract
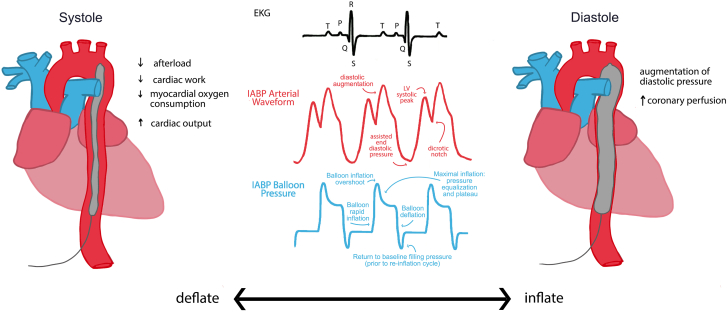
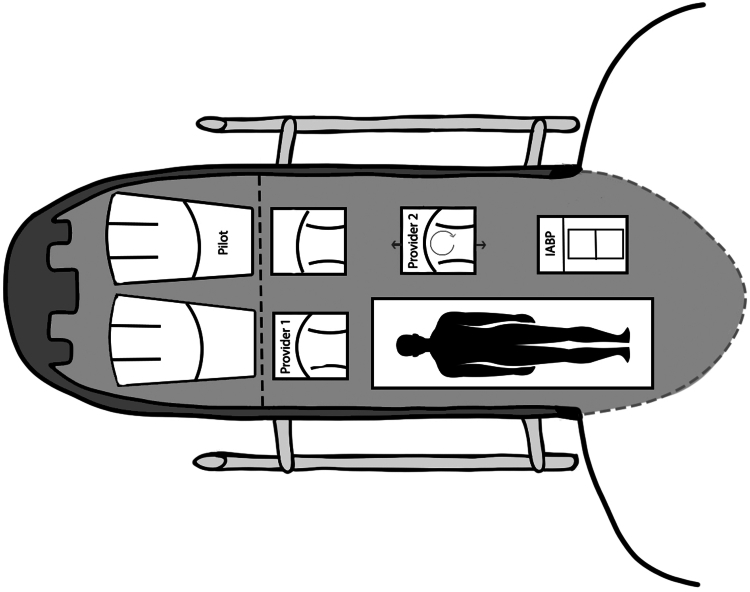
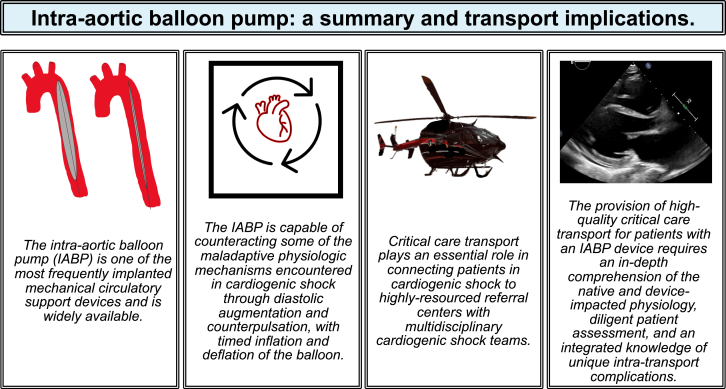
Critical care transport medicine (CCTM) teams are playing an increasing role in the care of patients in cardiogenic shock requiring mechanical circulatory support devices. Hence, it is important that CCTM providers are familiar with the pathophysiology of cardiogenic shock, the role of mechanical circulatory support, and the management of these devices in the transport environment. The intra-aortic balloon pump is a widely used and accessible cardiac support device capable of increasing cardiac output and reducing work on the left ventricle through diastolic augmentation and counterpulsation. This article reviews essential CCTM-based considerations for patients supported by intra-aortic balloon pump, including indications for placement, mechanics and physiology, potential issues during transport, and associated complications.
Keywords: cardiogenic shock; heart failure; mechanical circulatory support.
© 2024 The Author(s).
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
