

Changes in Left Ventricular Function and Outcomes After Trancatheter Edge-to-Edge Repair for Secondary Mitral Regurgitation
- PMID: 39132458
- PMCID: PMC11307461
- DOI: 10.1016/j.jscai.2024.101345
Changes in Left Ventricular Function and Outcomes After Trancatheter Edge-to-Edge Repair for Secondary Mitral Regurgitation
Erratum in
-
Correction.J Soc Cardiovasc Angiogr Interv. 2025 Aug 9;4(10Part A):103930. doi: 10.1016/j.jscai.2025.103930. eCollection 2025 Oct. J Soc Cardiovasc Angiogr Interv. 2025. PMID: 41268087 Free PMC article.
Abstract
Background: Transcatheter edge-to-edge repair (TEER) improved outcomes in patients with heart failure (HF) and severe secondary mitral regurgitation (SMR) compared with guideline-directed medical therapy (GDMT) alone regardless of the severity of baseline left ventricular ejection fraction (LVEF). The study aimed to evaluate the effect of early changes in LVEF after TEER and GDMT alone in patients with HF and severe SMR.
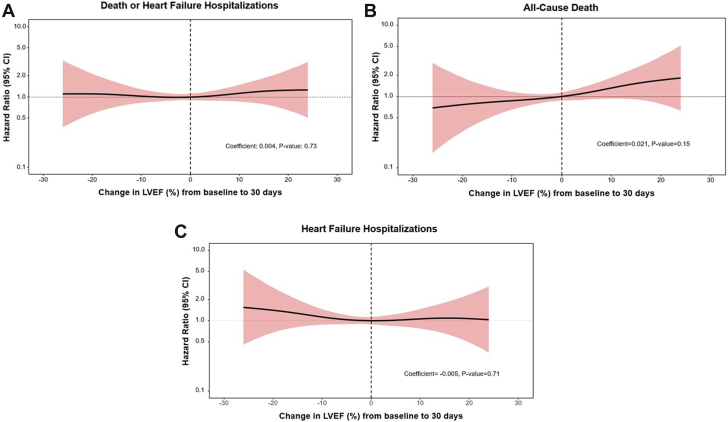
Methods: Within the COAPT trial, we evaluated outcomes according to changes in LVEF from baseline to 30 days. The primary outcome was all-cause death or HF hospitalization (HFH) between 30 days and 2 years.
Results: Among 432 patients with paired echocardiographic data, 182 (42.1%) had increased LVEF (LVEF change 6.0% ± 4.9%) and 250 (57.9%) had a decrease or no change in LVEF (LVEF change -6.6% ± 5.6%) from baseline to 30 days. LVEF at 30 days increased more frequently with GDMT alone compared with TEER plus GDMT (51.4% vs 33.0%; P = .0001). Between 30 days and 2 years, there were no significant differences in death or HFH in the increase LVEF and the decrease LVEF groups (58.8% vs 51.4%; multivariable-adjusted HR, 0.97; 95% CI, 0.87-1.08; P = .59). TEER plus GDMT reduced the 30-day to 2-year rate of death or HFH compared with GDMT alone consistently in patients with increase LVEF and decrease LVEF (Pint = 0.75).
Conclusions: Among patients with HF and severe SMR, early improvements in LVEF were more frequent with GDMT alone compared with TEER plus GDMT but were not associated with subsequent outcomes at 2 years. TEER reduced death or HFH during 2-year follow-up irrespective of early LVEF changes.
Keywords: GDMT; TEER; guideline-directed medical therapy; left ventricular ejection fraction; secondary mitral regurgitation; transcatheter edge-to-edge repair.
© 2024 The Author(s).
Figures



References
-
- Sannino A., Smith R.L., II, Schiattarella G.G., Trimarco B., Esposito G., Grayburn P.A. Survival and cardiovascular outcomes of patients with secondary mitral regurgitation: a systematic review and meta-analysis. JAMA Cardiol. 2017;2(10):1130–1139. doi: 10.1001/jamacardio.2017.2976. - DOI - PMC - PubMed
-
- Goel S.S., Bajaj N., Aggarwal B., et al. Prevalence and outcomes of unoperated patients with severe symptomatic mitral regurgitation and heart failure: comprehensive analysis to determine the potential role of MitraClip for this unmet need. J Am Coll Cardiol. 2014;63(2):185–186. doi: 10.1016/j.jacc.2013.08.723. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
