

Incidence of Mortality and Complications in High-Risk Pulmonary Embolism: A Systematic Review and Meta-Analysis
- PMID: 39132523
- PMCID: PMC11308857
- DOI: 10.1016/j.jscai.2022.100548
Incidence of Mortality and Complications in High-Risk Pulmonary Embolism: A Systematic Review and Meta-Analysis
Abstract
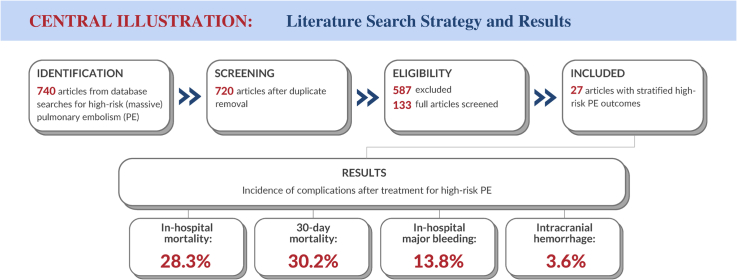
Background: The relationship between the early hemodynamic consequences of acute pulmonary embolism (PE) and short-term morbidity and mortality has long been recognized. The mortality incidence and other complications after high-risk (massive) PE, the most severe category of the disease, are summarized in this meta-analysis.
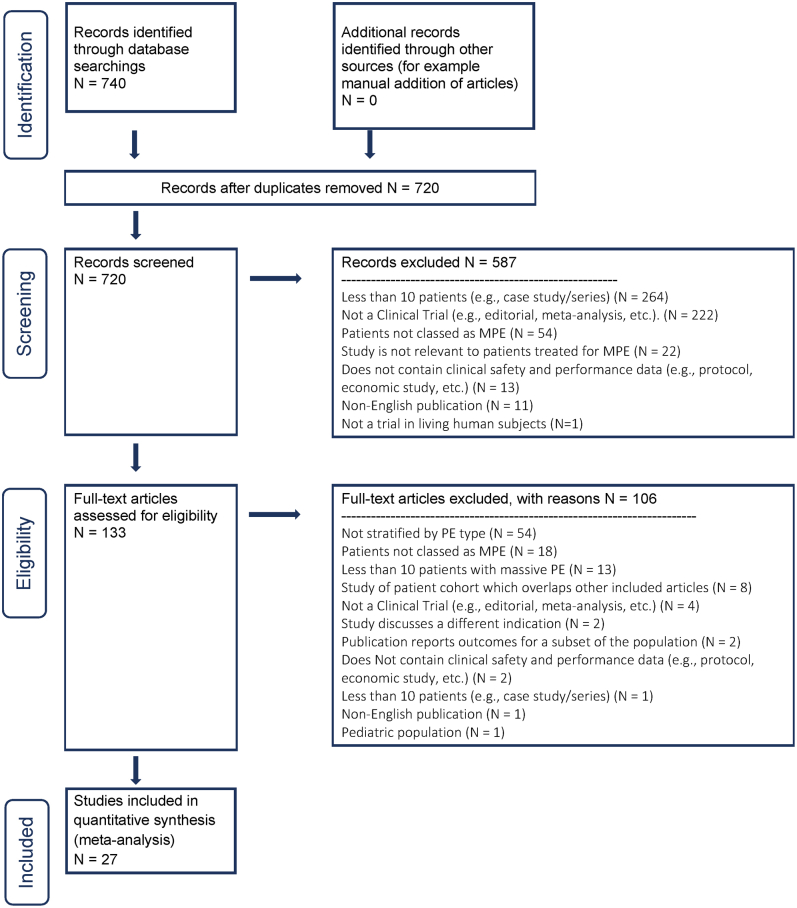
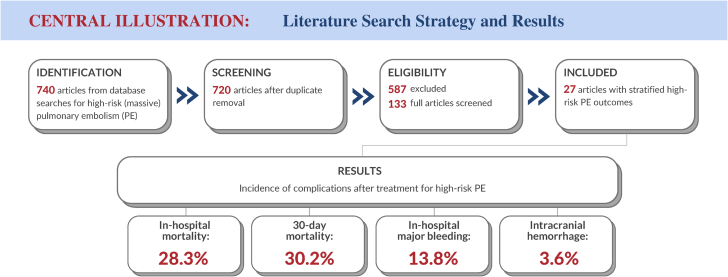
Methods: A systematic review and meta-analysis of studies reporting on patients with massive PE indexed by PubMed and the Cochrane Library over a 10-year period (2010-2020) was conducted. Studies with adequate information to specify a cohort of patients with high-risk PE defined by the American Heart Association and European Society of Cardiology criteria and their clinical outcomes were included. Incidences were calculated as weighted averages with 95% CIs.
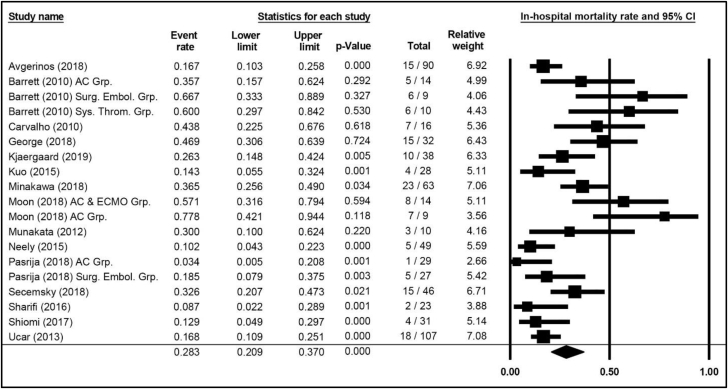
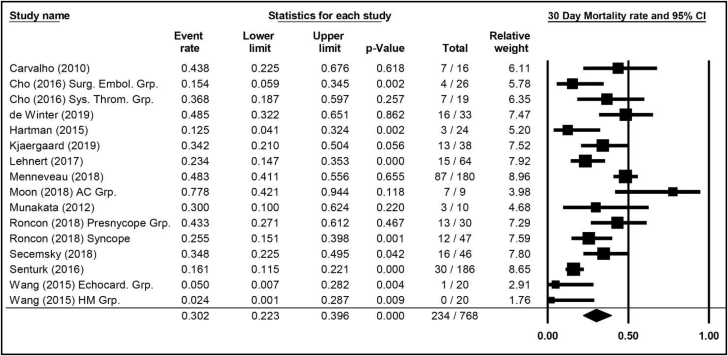
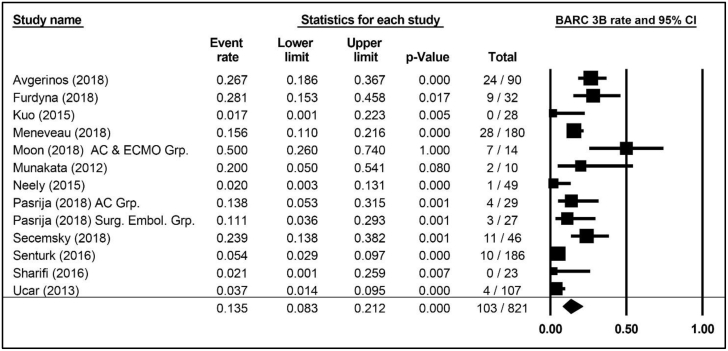
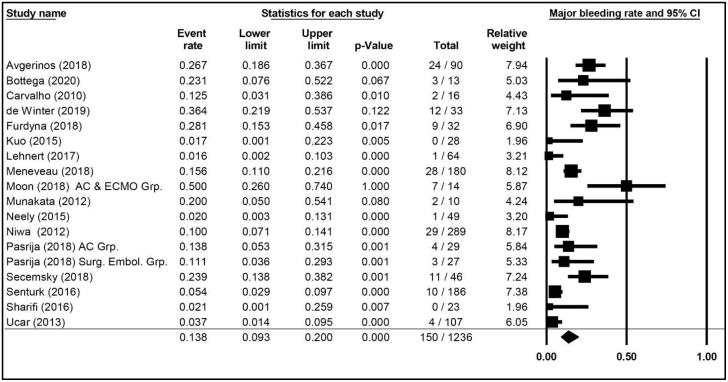
Results: A total of 27 publications spanning 1517 patients were identified that met the search criteria for high-risk PE. In-hospital all-cause mortality averaged 28.3% (95% CI, 20.9%-37.0%) in patients at high risk, comparable to the 30-day all-cause mortality of 30.2% (95% CI, 22.3%-39.6%). In-hospital major bleeding was 13.8% (95% CI, 9.3%-20.0%), and intracranial hemorrhage was reported in 3.6% (95% CI, 2.2%-5.9%). The risk of bias in publications was graded as low-to-moderate, with substantial heterogeneity among the studies.
Conclusions: This systematic review and meta-analysis provided low-quality to moderate-quality evidence documenting mortality, major bleeding, and other complications in patients meeting the American Heart Association and European Society of Cardiology criteria for high-risk PE. This information was used to inform the design of the FLowTriever for Acute Massive Pulmonary Embolism (FLAME) study (NCT04795167), a study evaluating an advanced therapy for patients with high-risk PE.
Keywords: high-risk; massive; mechanical thrombectomy; pulmonary embolism; thromboembolectomy; thrombolysis.
© 2022 The Authors.
Figures
References
-
- Prabhu W., Soukas P.A. Pulmonary embolism in 2017: increasing options for increasing incidence. R I Med J (2013) 2017;100(5):27–32. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
