

Combination of Hydrogen Inhalation and Hypothermic Temperature Control After Out-of-Hospital Cardiac Arrest: A Post hoc Analysis of the Efficacy of Inhaled Hydrogen on Neurologic Outcome Following Brain Ischemia During PostCardiac Arrest Care II Trial
- PMID: 39133068
- PMCID: PMC11392137
- DOI: 10.1097/CCM.0000000000006395
Combination of Hydrogen Inhalation and Hypothermic Temperature Control After Out-of-Hospital Cardiac Arrest: A Post hoc Analysis of the Efficacy of Inhaled Hydrogen on Neurologic Outcome Following Brain Ischemia During PostCardiac Arrest Care II Trial
Abstract
Objective: The Efficacy of Inhaled Hydrogen on Neurologic Outcome Following Brain Ischemia During Post-Cardiac Arrest Care (HYBRID) II trial (jRCTs031180352) suggested that hydrogen inhalation may reduce post-cardiac arrest brain injury (PCABI). However, the combination of hypothermic target temperature management (TTM) and hydrogen inhalation on outcomes is unclear. The aim of this study was to investigate the combined effect of hydrogen inhalation and hypothermic TTM on outcomes after out-of-hospital cardiac arrest (OHCA).
Design: Post hoc analysis of a multicenter, randomized, controlled trial.
Setting: Fifteen Japanese ICUs.
Patients: Cardiogenic OHCA enrolled in the HYBRID II trial.
Interventions: Hydrogen mixed oxygen (hydrogen group) versus oxygen alone (control group).
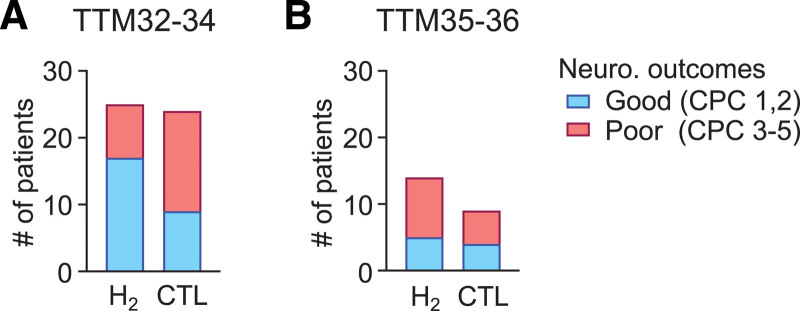
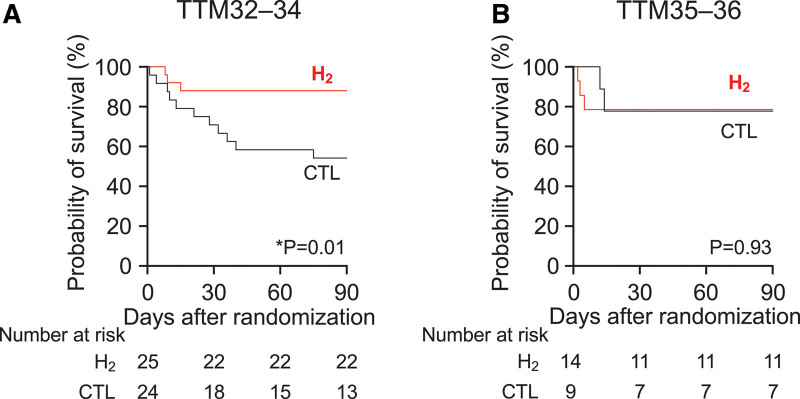
Measurements and main results: TTM was performed at a target temperature of 32-34°C (TTM32-TTM34) or 35-36°C (TTM35-TTM36) per the institutional protocol. The association between hydrogen + TTM32-TTM34 and 90-day good neurologic outcomes was analyzed using generalized estimating equations. The 90-day survival was compared between the hydrogen and control groups under TTM32-TTM34 and TTM35-TTM36, respectively. The analysis included 72 patients (hydrogen [ n = 39] and control [ n = 33] groups) with outcome data. TTM32-TTM34 was implemented in 25 (64%) and 24 (73%) patients in the hydrogen and control groups, respectively ( p = 0.46). Under TTM32-TTM34, 17 (68%) and 9 (38%) patients achieved good neurologic outcomes in the hydrogen and control groups, respectively (relative risk: 1.81 [95% CI, 1.05-3.66], p < 0.05). Hydrogen + TTM32-TTM34 was independently associated with good neurologic outcomes (adjusted odds ratio 16.10 [95% CI, 1.88-138.17], p = 0.01). However, hydrogen + TTM32-TTM34 did not improve survival compared with TTM32-TTM34 alone (adjusted hazard ratio: 0.22 [95% CI, 0.05-1.06], p = 0.06).
Conclusions: Hydrogen + TTM32-TTM34 was associated with improved neurologic outcomes after cardiogenic OHCA compared with TTM32-TTM34 monotherapy. Hydrogen inhalation is a promising treatment option for reducing PCABI when combined with TTM32-TTM34.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine and Wolters Kluwer Health, Inc.
Conflict of interest statement
Dr. Tamura’s institution received funding from the Taiyo Nippon Sanso Corporation, the Japanese Society for Promotion of Science, and the Marumo Memorial Foundation Grant for Emergency Medicine Research. Drs. Tamura and Suzuki disclosed off-label use of hydrogen gas. Dr. Narumiya disclosed work for hire. Dr. Homma has disclosed that he does not have any potential conflicts of interest.
Figures

Similar articles
-
Efficacy of inhaled HYdrogen on neurological outcome following BRain Ischemia During post-cardiac arrest care (HYBRID II trial): study protocol for a randomized controlled trial.Trials. 2017 Oct 23;18(1):488. doi: 10.1186/s13063-017-2246-3. Trials. 2017. PMID: 29058596 Free PMC article. Clinical Trial.
-
Differential Effect of Targeted Temperature Management Between 32 °C and 36 °C Following Cardiac Arrest According to Initial Severity of Illness: Insights From Two International Data Sets.Chest. 2023 May;163(5):1120-1129. doi: 10.1016/j.chest.2022.10.023. Epub 2022 Oct 30. Chest. 2023. PMID: 36445800
-
Long-term survival in out-of-hospital cardiac arrest patients treated with targeted temperature control at 33 °C or 36 °C: A national registry study.Resuscitation. 2019 Oct;143:142-147. doi: 10.1016/j.resuscitation.2019.08.029. Epub 2019 Aug 27. Resuscitation. 2019. PMID: 31470100
-
Targeted Temperature Management for 48 vs 24 Hours and Neurologic Outcome After Out-of-Hospital Cardiac Arrest: A Randomized Clinical Trial.JAMA. 2017 Jul 25;318(4):341-350. doi: 10.1001/jama.2017.8978. JAMA. 2017. PMID: 28742911 Free PMC article. Clinical Trial.
-
Biomarkers in Cardiac Arrest: A Narrative Review.Ther Adv Pulm Crit Care Med. 2025 Jun 4;20:29768675251346014. doi: 10.1177/29768675251346014. eCollection 2025 Jan-Dec. Ther Adv Pulm Crit Care Med. 2025. PMID: 40475878 Free PMC article. Review.
Cited by
-
Pharmacokinetics of Hydrogen During Hydrogen-Saturated Saline Infusion in Pigs.Biomedicines. 2025 Jan 19;13(1):234. doi: 10.3390/biomedicines13010234. Biomedicines. 2025. PMID: 39857817 Free PMC article.
-
Molecular Hydrogen Therapy: Mechanisms, Delivery Methods, Preventive, and Therapeutic Application.MedComm (2020). 2025 Apr 28;6(5):e70194. doi: 10.1002/mco2.70194. eCollection 2025 May. MedComm (2020). 2025. PMID: 40297245 Free PMC article. Review.
References
-
- Nishiyama C, Kiguchi T, Okubo M, et al. : Three-year trends in out-of-hospital cardiac arrest across the world: Second report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation. 2023; 186:109757. - PubMed
-
- Perkins GD, Callaway CW, Haywood K, et al. : Brain injury after cardiac arrest. Lancet. 2021; 398:1269–1278 - PubMed
-
- Perman SM, Bartos JA, Del Rios M, et al. ; American Heart Association Emergency Cardiovascular Care Committee, Council on Cardiovascular Surgery and Anesthesia; Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Peripheral Vascular Disease; Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, and Stroke Council: Temperature management for comatose adult survivors of cardiac arrest: A science advisory from the American Heart Association. Circulation. 2023; 148:982–988 - PubMed
-
- Ohsawa I, Ishikawa M, Takahashi K, et al. : Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat Med. 2007; 13:688–694 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
