

Real-world experience with CDK4/6 inhibitors in hormone receptor-positive metastatic and recurrent breast cancer: findings from an Asian population
- PMID: 39133334
- PMCID: PMC11319386
- DOI: 10.1007/s10238-024-01458-1
Real-world experience with CDK4/6 inhibitors in hormone receptor-positive metastatic and recurrent breast cancer: findings from an Asian population
Abstract
Purpose: Cyclin-dependent kinase 4/6 inhibitors (CDK4/6i) combined with endocrine therapy have demonstrated significant clinical benefits in progression-free and overall survival. This study investigates the outcomes associated with two kinds of CDK4/6i in patients with hormone receptor (HR)-positive metastatic and relapsed breast cancer to inform real-world evidence of treatment strategies.
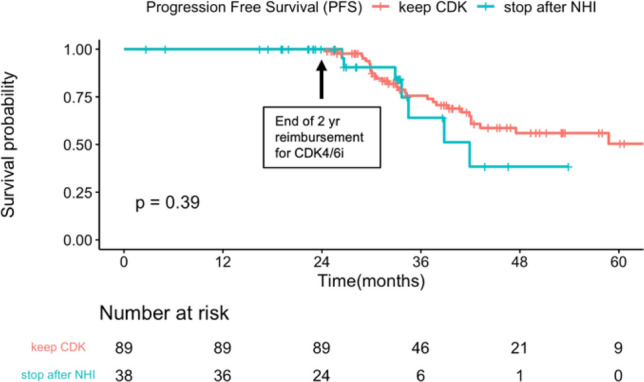
Methods: This retrospective study included 340 Taiwanese patients with HR-positive advanced breast cancer from the Taipei Veterans General Hospital, between 2018 and 2023. We analyzed patient characteristics, treatment strategies and outcomes associated with two CDK4/6i. The efficacy of patients who experienced economic burden and interrupted CDK4/6i treatment after 2 years of National Health Insurance (NHI) reimbursement was also investigated.
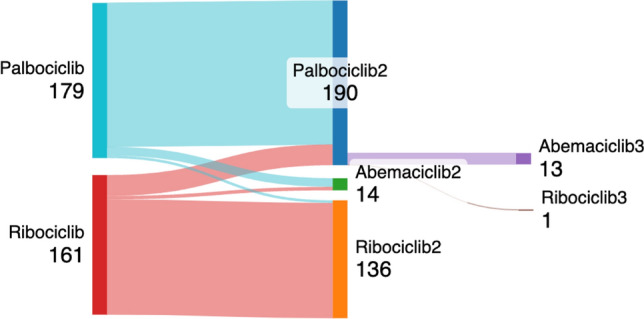
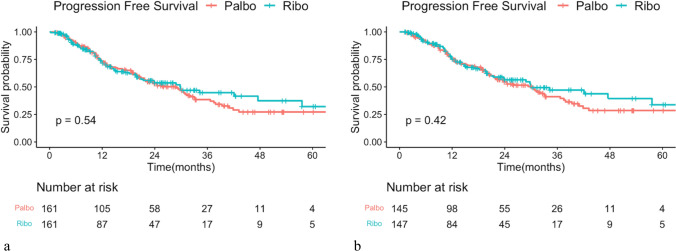
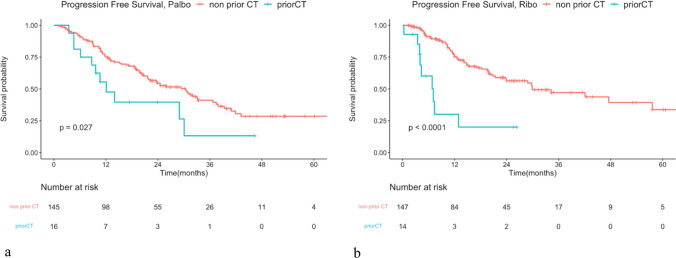
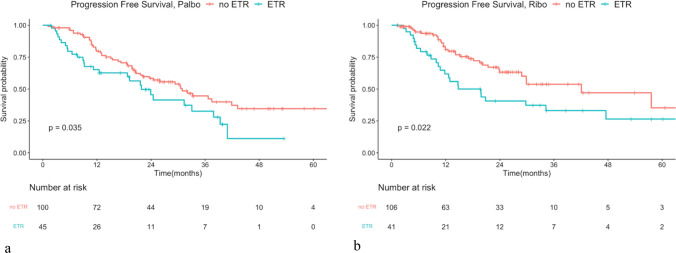
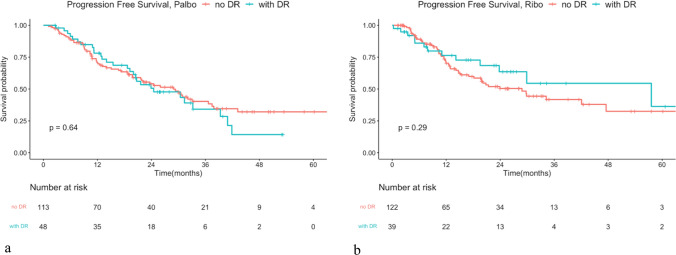
Results: Patients receiving ribociclib and palbociclib showed no significant differences in age, histology, body mass index(BMI), or pathologic status. The distribution of disease status and endocrine therapy partners was comparable between the two groups. Dose reduction was similar, while patients with palbociclib tended to discontinue CDK4/6i usage, and those with ribociclib tended to switch to the other CDK4/6i or endocrine partners. There was no significant difference in progression-free survival (PFS) between the two CDK4/6i in the first-line setting. Adverse prognostic factors were increasing HER2 IHC score, higher Ki-67 levels, visceral and liver metastasis, prior chemotherapy, and endocrine therapy resistance, while higher BMI, bone-only metastasis, and letrozole treatment were associated with a lower risk of progression. The limited follow-up time in our study was insufficient to assess the outcomes of patients treated with interrupted CDK4/6i for up to two years under the NHI reimbursement policy.
Conclusion: Treatment outcomes between the two types of CDK4/6i did not differ significantly, indicating the safety and efficacy of CDK4/6i for the Asian population. Ribociclib and palbociclib showed similar efficacy in PFS in the real-world setting.
Keywords: Breast cancer; CDK4/6 inhibitors; Real-world data; Taiwanese; Treatment outcomes.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
