

Chronic Airflow Limitation, Emphysema, and Impaired Diffusing Capacity in Relation to Smoking Habits in a Swedish Middle-aged Population
- PMID: 39133529
- PMCID: PMC11622819
- DOI: 10.1513/AnnalsATS.202402-122OC
Chronic Airflow Limitation, Emphysema, and Impaired Diffusing Capacity in Relation to Smoking Habits in a Swedish Middle-aged Population
Abstract
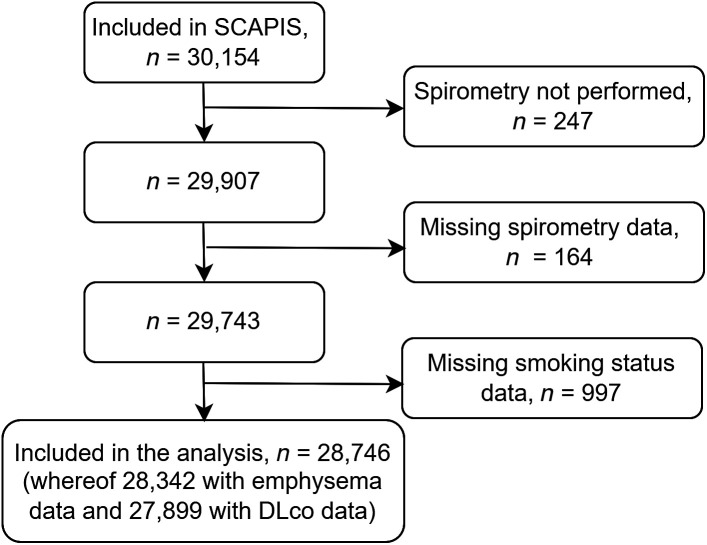
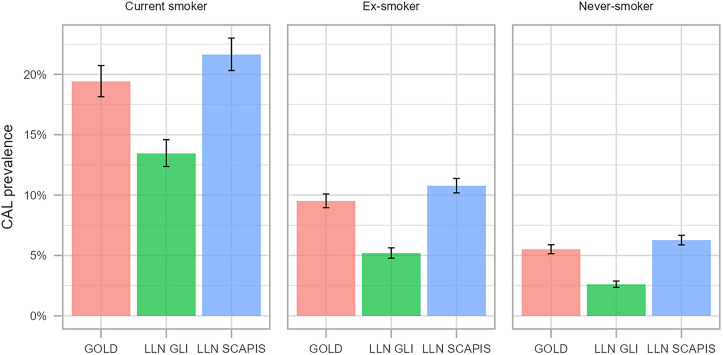
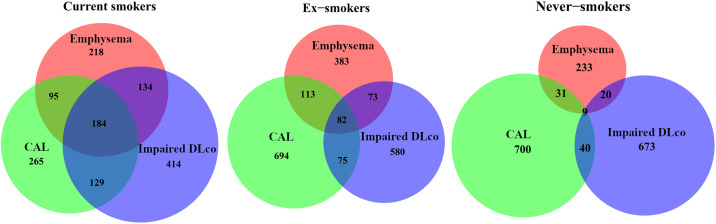
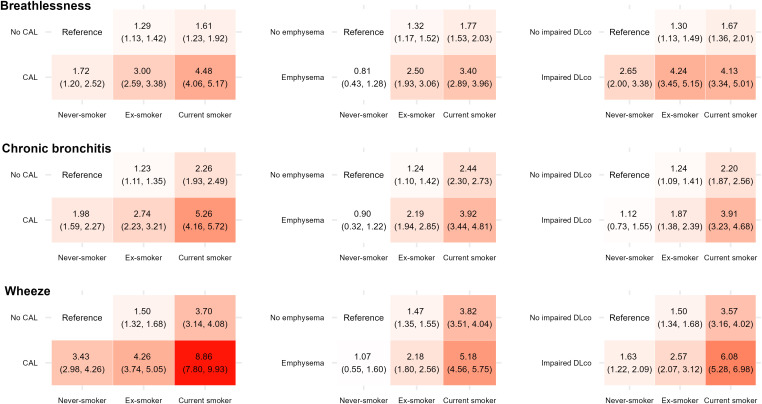
Rationale: Chronic obstructive pulmonary disease (COPD) includes respiratory symptoms and chronic airflow limitation (CAL). In some cases, emphysema and impaired diffusing capacity of the lung for carbon monoxide (DlCO) are present, but characteristics and symptoms vary with smoking exposure. Objective: To study the prevalence of CAL, emphysema, and impaired DlCO in relation to smoking and respiratory symptoms in a middle-aged population. Methods: We investigated 28,746 randomly invited individuals (52% women) aged 50-64 years across six Swedish sites. We performed spirometry, DlCO testing, and high-resolution computed tomography and asked for smoking habits and respiratory symptoms. CAL was defined as post-bronchodilator forced expiratory volume in 1 second divided by forced vital capacity (FEV1/FVC) < 0.7. Results: The overall prevalence was 8.8% for CAL, 5.7% for impaired DlCO (DlCO < LLN), and 8.8% for emphysema, with a higher prevalence in current smokers than in ex-smokers and never-smokers. The proportion of never-smokers among those with CAL, emphysema, and impaired DlCO was 32%, 19%, and 31%, respectively. Regardless of smoking habits, the prevalence of respiratory symptoms was higher among people with CAL and impaired DlCO than those with normal lung function. Asthma prevalence in never-smokers with CAL was 14%. In this group, asthma was associated with lower FEV1 and more respiratory symptoms. Conclusions: In this large population-based study of middle-aged people, CAL and impaired DlCO were associated with common respiratory symptoms. Self-reported asthma was not associated with CAL in never-smokers. Our findings suggest that CAL in never-smokers signifies a separate clinical phenotype that may be monitored and, possibly, treated differently from smoking-related COPD.
Keywords: chronic obstructive pulmonary disease; emphysema; impaired DlCO; respiratory symptoms; smoking.
Figures
Comment in
-
Chronic Airflow Limitation in Never-Smokers: Time to Broaden Our Focus beyond Smoking in Chronic Obstructive Pulmonary Disease.Ann Am Thorac Soc. 2024 Dec;21(12):1653-1654. doi: 10.1513/AnnalsATS.202410-1018ED. Ann Am Thorac Soc. 2024. PMID: 39601501 Free PMC article. No abstract available.
References
-
- Çolak Y, Afzal S, Nordestgaard BG, Vestbo J, Lange P. Prognosis of asymptomatic and symptomatic, undiagnosed COPD in the general population in Denmark: a prospective cohort study. Lancet Respir Med . 2017;5:426–434. - PubMed
-
- Brisman J, Kim JL, Olin AC, Torén K, Bake B. Spirometric reference equations for Swedish adults. Clin Physiol Funct Imaging . 2017;37:640–645. - PubMed
-
- Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM, et al. BOLD Collaborative Research Group International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet . 2007;370:741–750. - PubMed
Publication types
MeSH terms
Grants and funding
- Hjärt-Lungfonden/United States
- Knut och Alice Wallenbergs Stiftelse/United States
- Vetenskapsrådet/United States
- VINNOVA/United States
- Göteborgs Universitet/United States
- Sahlgrenska Universitetssjukhuset/United States
- Karolinska Institutet/United States
- Stockholm läns landsting/United States
- Linköpings Universitet/United States
- Linköping University Hospital/United States
- Lunds Universitet/United States
- Skånes universitetssjukhus/United States
- Umeå Universitet/United States
- Uppsala Universitet/United States
- Akademiska Sjukhuset/United States
LinkOut - more resources
Full Text Sources
Medical
