

Differentiation of Prior SARS-CoV-2 Infection and Postacute Sequelae by Standard Clinical Laboratory Measurements in the RECOVER Cohort
- PMID: 39133923
- PMCID: PMC11408082
- DOI: 10.7326/M24-0737
Differentiation of Prior SARS-CoV-2 Infection and Postacute Sequelae by Standard Clinical Laboratory Measurements in the RECOVER Cohort
Abstract
Background: There are currently no validated clinical biomarkers of postacute sequelae of SARS-CoV-2 infection (PASC).
Objective: To investigate clinical laboratory markers of SARS-CoV-2 and PASC.
Design: Propensity score-weighted linear regression models were fitted to evaluate differences in mean laboratory measures by prior infection and PASC index (≥12 vs. 0). (ClinicalTrials.gov: NCT05172024).
Setting: 83 enrolling sites.
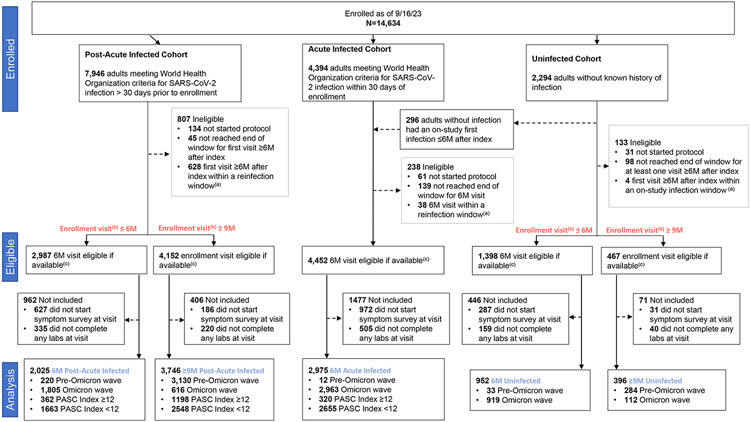
Participants: RECOVER-Adult cohort participants with or without SARS-CoV-2 infection with a study visit and laboratory measures 6 months after the index date (or at enrollment if >6 months after the index date). Participants were excluded if the 6-month visit occurred within 30 days of reinfection.
Measurements: Participants completed questionnaires and standard clinical laboratory tests.
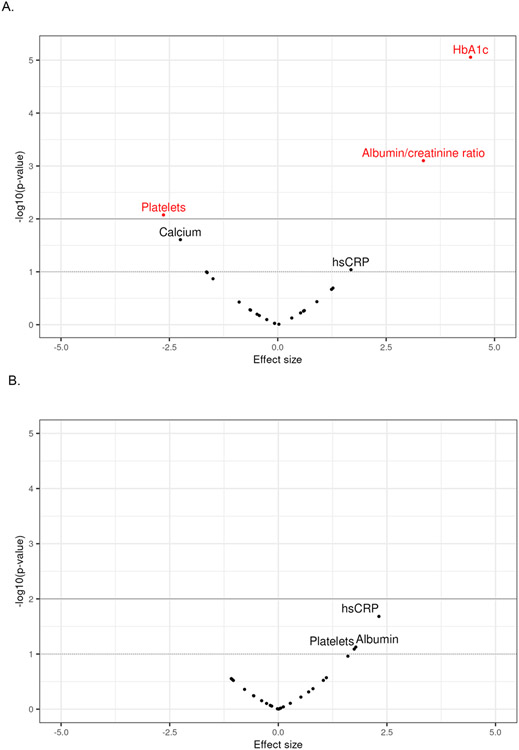
Results: Among 10 094 participants, 8746 had prior SARS-CoV-2 infection, 1348 were uninfected, 1880 had a PASC index of 12 or higher, and 3351 had a PASC index of zero. After propensity score adjustment, participants with prior infection had a lower mean platelet count (265.9 × 109 cells/L [95% CI, 264.5 to 267.4 × 109 cells/L]) than participants without known prior infection (275.2 × 109 cells/L [CI, 268.5 to 282.0 × 109 cells/L]), as well as higher mean hemoglobin A1c (HbA1c) level (5.58% [CI, 5.56% to 5.60%] vs. 5.46% [CI, 5.40% to 5.51%]) and urinary albumin-creatinine ratio (81.9 mg/g [CI, 67.5 to 96.2 mg/g] vs. 43.0 mg/g [CI, 25.4 to 60.6 mg/g]), although differences were of modest clinical significance. The difference in HbA1c levels was attenuated after participants with preexisting diabetes were excluded. Among participants with prior infection, no meaningful differences in mean laboratory values were found between those with a PASC index of 12 or higher and those with a PASC index of zero.
Limitation: Whether differences in laboratory markers represent consequences of or risk factors for SARS-CoV-2 infection could not be determined.
Conclusion: Overall, no evidence was found that any of the 25 routine clinical laboratory values assessed in this study could serve as a clinically useful biomarker of PASC.
Primary funding source: National Institutes of Health.
Conflict of interest statement
Figures
References
-
- ;PagesGenerated interactively: from https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm on 1/February/2024.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous