

Performance of amide proton transfer imaging to differentiate true progression from therapy-related changes in gliomas and metastases
- PMID: 39134744
- PMCID: PMC11782315
- DOI: 10.1007/s00330-024-11004-y
Performance of amide proton transfer imaging to differentiate true progression from therapy-related changes in gliomas and metastases
Abstract
Objectives: Differentiating true progression or recurrence (TP/TR) from therapy-related changes (TRC) is complex in brain tumours. Amide proton transfer-weighted (APT) imaging is a chemical exchange saturation transfer (CEST) MRI technique that may improve diagnostic accuracy during radiological follow-up. This systematic review and meta-analysis elucidated the level of evidence and details of state-of-the-art imaging for APT-CEST in glioma and brain metastasis surveillance.
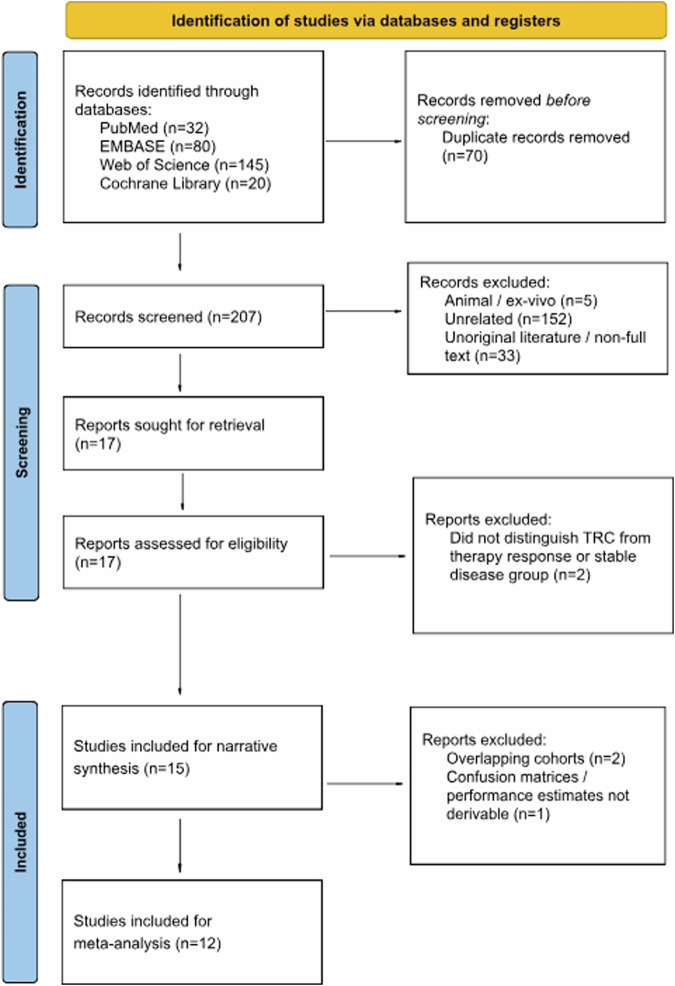
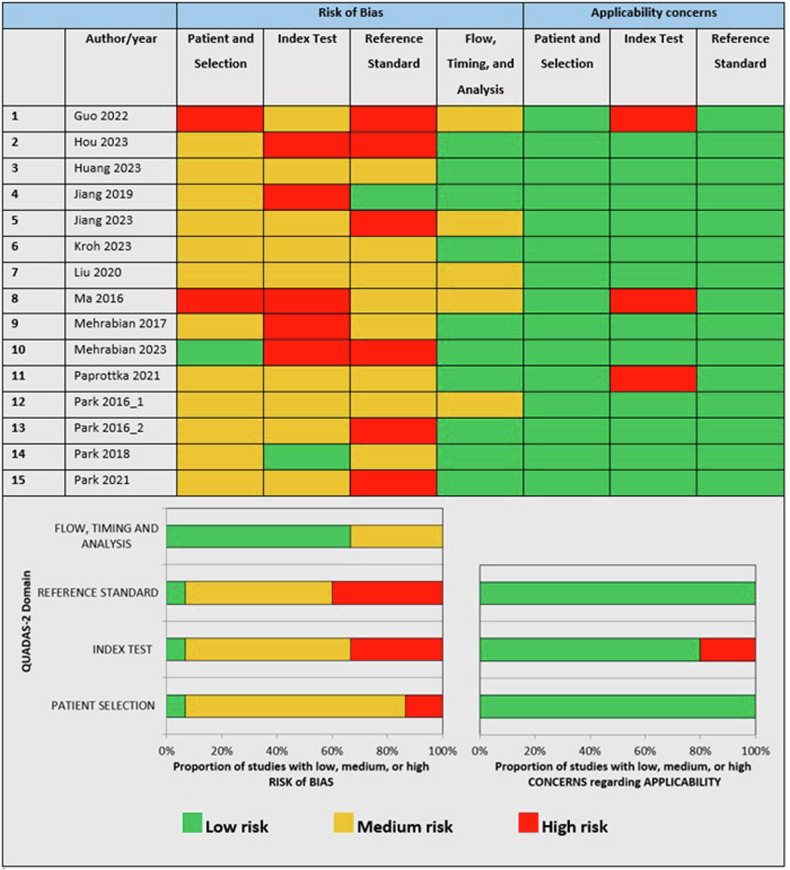
Methods: PubMed, EMBASE, Web of Science, and Cochrane Library were systematically searched for original articles about glioma and metastasis patients who received APT-CEST imaging for suspected TP/TR within 2 years after (chemo)radiotherapy completion. Modified Quality Assessment of Diagnostic Accuracy Studies-2 criteria were applied. A meta-analysis was performed to pool results and to compare subgroups.
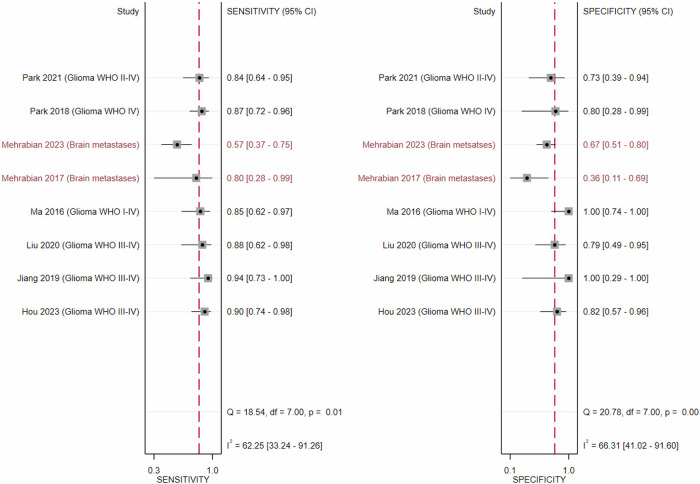
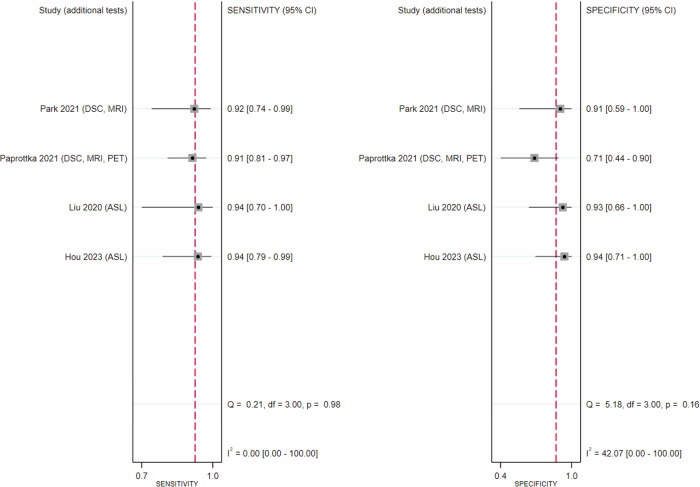
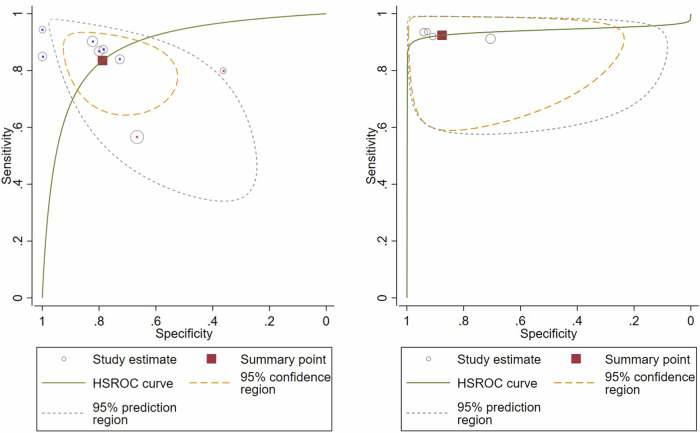
Results: Fifteen studies were included for a narrative synthesis, twelve of which (500 patients) were deemed sufficiently homogeneous for a meta-analysis. Magnetisation transfer ratio asymmetry performed well in gliomas (sensitivity 0.88 [0.82-0.92], specificity 0.84 [0.72-0.91]) but not in metastases (sensitivity 0.64 [0.38-0.84], specificity 0.56 [0.33-0.77]). APT-CEST combined with conventional/advanced MRI rendered 0.92 [0.86-0.96] and 0.88 [0.72-0.95] in gliomas. Tumour type, TR prevalence, sex, and acquisition protocol were sources of significant inter-study heterogeneity in sensitivity (I2 = 62.25%; p < 0.01) and specificity (I2 = 66.31%; p < 0.001).
Conclusion: A growing body of literature suggests that APT-CEST is a promising technique for improving the discrimination of TP/TR from TRC in gliomas, with limited data on metastases.
Clinical relevance statement: This meta-analysis identified a utility for APT-CEST imaging regarding the non-invasive discrimination of brain tumour progression from therapy-related changes, providing a critical evaluation of sequence parameters and cut-off values, which can be used to improve response assessment and patient outcome.
Key points: Therapy-related changes mimicking progression complicate brain tumour treatment. Amide proton imaging improves the non-invasive discrimination of glioma progression from therapy-related changes. Magnetisation transfer ratio asymmetry measurement seems not to have added value in brain metastases.
Keywords: Brain metastasis; Glioma; Magnetic resonance imaging; Molecular imaging; Therapy response.
© 2024. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is V.C.K. Conflict of interest: V.C.K. is a Junior Deputy Editor for European Radiology. They have not participated in the selection or review processes. The remaining authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. Statistics and biometry: One of the authors has significant statistical expertise. Informed consent: Written informed consent was not required for this study because of the study type. Ethical approval: Institutional Review Board approval was not required because it is not necessary for a review. Study subjects or cohorts overlap: Some study subjects or cohorts have been previously reported in the cited source articles (as is normal for a systematic review). Methodology: Retrospective Multicenter study
Figures
References
-
- Lacerda S, Barisano G, Shiroishi MS, Law M (2023) Clinical applications of dynamic contrast-enhanced (DCE) permeability imaging. In: Faro SH, Mohamed FB (eds) Functional neuroradiology: principles and clinical applications. Springer, Cham, 175–200
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
