

Redefining urine output thresholds for acute kidney injury criteria in critically Ill patients: a derivation and validation study
- PMID: 39135063
- PMCID: PMC11321122
- DOI: 10.1186/s13054-024-05054-3
Redefining urine output thresholds for acute kidney injury criteria in critically Ill patients: a derivation and validation study
Abstract
Introduction: The current definition of acute kidney injury (AKI) includes increased serum creatinine (sCr) concentration and decreased urinary output (UO). Recent studies suggest that the standard UO threshold of 0.5 ml/kg/h may be suboptimal. This study aimed to develop and validate a novel UO-based AKI classification system that improves mortality prediction and patient stratification.
Methods: Data were obtained from the MIMIC-IV and eICU databases. The development process included (1) evaluating UO as a continuous variable over 3-, 6-, 12-, and 24-h periods; (2) identifying 3 optimal UO cutoff points for each time window (stages 1, 2, and 3); (3) comparing sensitivity and specificity to develop a unified staging system; (4) assessing average versus persistent reduced UO hourly; (5) comparing the new UO-AKI system to the KDIGO UO-AKI system; (6) integrating sCr criteria with both systems and comparing them; and (7) validating the new classification with an independent cohort. In all these steps, the outcome was hospital mortality. Another analyzed outcome was 90-day mortality. The analyses included ROC curve analysis, net reclassification improvement (NRI), integrated discrimination improvement (IDI), and logistic and Cox regression analyses.
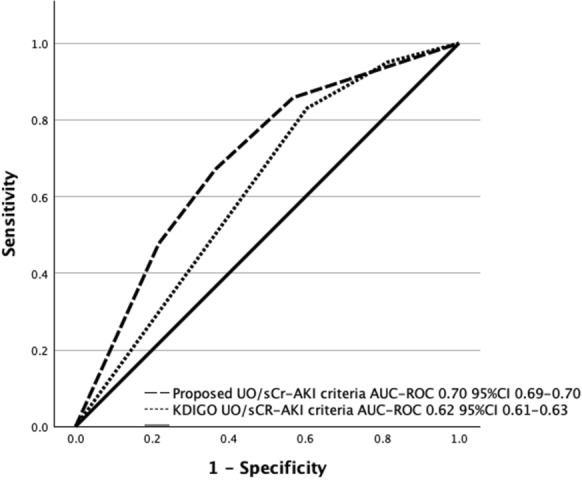
Results: From the MIMIC-IV database, 35,845 patients were included in the development cohort. After comparing the sensitivity and specificity of 12 different lowest UO thresholds across four time frames, 3 cutoff points were selected to compose the proposed UO-AKI classification: stage 1 (0.2-0.3 mL/kg/h), stage 2 (0.1-0.2 mL/kg/h), and stage 3 (< 0.1 mL/kg/h) over 6 h. The proposed classification had better discrimination when the average was used than when the persistent method was used. The adjusted odds ratio demonstrated a significant stepwise increase in hospital mortality with advancing UO-AKI stage. The proposed classification combined or not with the sCr criterion outperformed the KDIGO criteria in terms of predictive accuracy-AUC-ROC 0.75 (0.74-0.76) vs. 0.69 (0.68-0.70); NRI: 25.4% (95% CI: 23.3-27.6); and IDI: 4.0% (95% CI: 3.6-4.5). External validation with the eICU database confirmed the superior performance of the new classification system.
Conclusion: The proposed UO-AKI classification enhances mortality prediction and patient stratification in critically ill patients, offering a more accurate and practical approach than the current KDIGO criteria.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Comment in
-
New definition of AKI: shifting the focus beyond mortality.Crit Care. 2024 Nov 20;28(1):379. doi: 10.1186/s13054-024-05170-0. Crit Care. 2024. PMID: 39568083 Free PMC article. No abstract available.
-
Structural, physiological or clinical outcomes to define urine output threshold in acute kidney injury.Crit Care. 2024 Dec 18;28(1):410. doi: 10.1186/s13054-024-05195-5. Crit Care. 2024. PMID: 39695747 Free PMC article. No abstract available.
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl (2011). 2012;2(1):1–138. 10.1038/kisup.2012.6
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
