

Systematic literature review of the somatic comorbidities experienced by adults with phenylketonuria
- PMID: 39135125
- PMCID: PMC11318169
- DOI: 10.1186/s13023-024-03203-z
Systematic literature review of the somatic comorbidities experienced by adults with phenylketonuria
Abstract
Background: Phenylketonuria (PKU) is an inborn error of phenylalanine (Phe) metabolism that, if untreated, causes Phe accumulation in the brain leading to neurophysiologic alterations and poor outcomes. Lifelong management centers on dietary Phe restriction, yet long-term complete metabolic control is unachievable for many adults. High blood Phe levels or chronic Phe and intact protein restriction in the diet may lead to somatic comorbidities. A systematic literature review was conducted to evaluate somatic comorbidities experienced by adults with PKU.
Methods: Clinical and observational studies reporting somatic comorbidities experienced by individuals with PKU aged ≥ 16 years (or classified as adults) evaluating a Phe-restricted diet with or without pharmacologic therapy versus no therapeutic intervention (including healthy controls), or pharmacologic therapy versus a Phe-restricted diet alone, were identified. PubMed® was searched (February 1, 2022 and updated November 1, 2023), using a pre-defined search strategy, followed by two-stage screening and data extraction. Included studies were grouped by PKU population comparison.
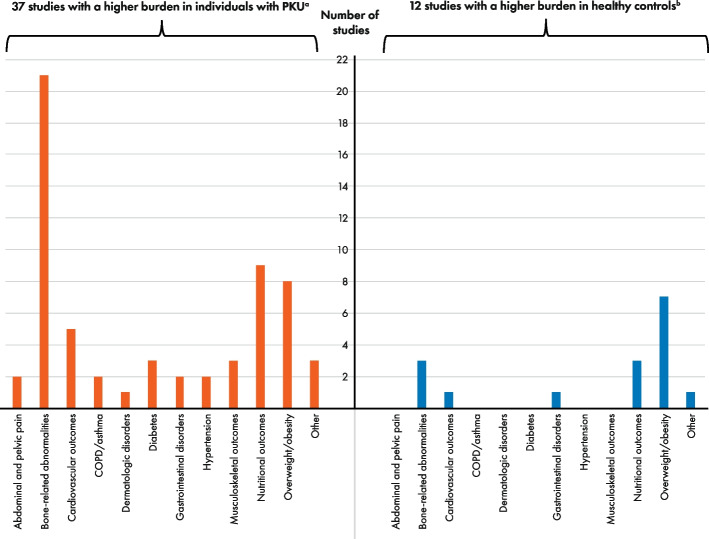
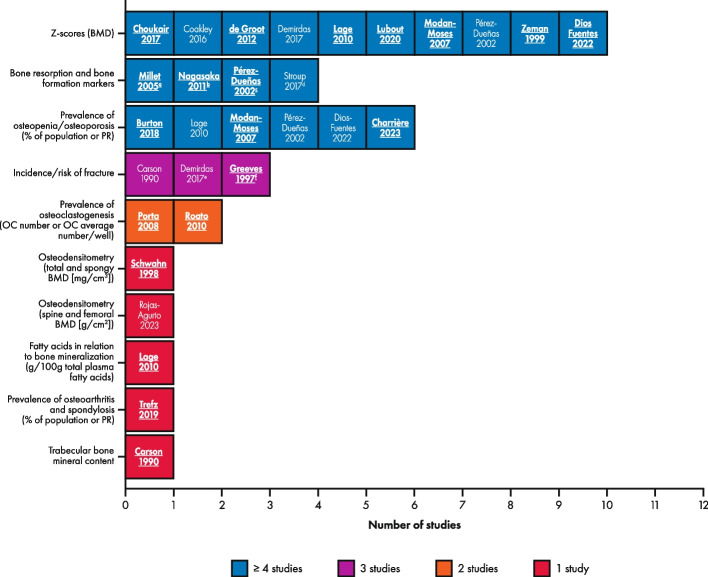
Results: 1185 records were screened; 51 studies across 12,602 individuals were extracted. Bone-related abnormalities were the most reported outcome (n = 21); several outcome measures were used. Original study groupings included: Phe-restricted diet versus healthy controls or reference values (n = 40); treatment-adherent versus those non-adherent (n = 12). Additional groups added as part of a protocol amendment included: different Phe-restricted diets (n = 4); severe versus less severe disease (n = 5). Vote counting indicated a higher burden of ≥ 1 comorbidity (or outcome measure) for the Phe-restricted diet group by 37 of 38 studies included in the analysis of Phe-restricted diet versus healthy controls; higher burden in healthy controls was reported in 12 studies. Vote counting was similar between those treatment adherent (n = 7) versus non-adherent (n = 10).
Conclusions: Adults with PKU have a higher comorbidity burden than a non-PKU population. More robust studies are needed to better understand the relationship between effective metabolic control and comorbidity burden, using consistent outcome measures. This SLR was supported by BioMarin Pharmaceutical Inc., Novato, CA, and is registered with the Research Registry (reviewregistry1476).
Keywords: Adherence; Comorbidity; Diet; Disease burden; Nutritional status; Phenylalanine; Phenylalanine hydroxylase; Phenylketonuria; Systematic review.
© 2024. The Author(s).
Conflict of interest statement
KBW, SR, and GEC are employees and stockholders of BioMarin. KKA has received consulting payments from Arla Foods Ingredients, BioMarin, Homology, and Nutricia. DAB has received consulting payments from BioMarin, Encoded Therapeutics, Synlogic Therapeutics, and Taysha Gene Therapies, and travel support from BioMarin. COH has received consulting and speaker fees/payments from BioMarin and has participated as a clinical trial investigator for BioMarin. AH has received consulting payments from Amicus Therapeutics, BioMarin, Chiesi, Genzyme, Shire, and Ultragenyx; speaker fees/payments from Alexion, Amicus Therapeutics, BioMarin, Genzyme, InMedica, Nutricia, Sobi, Takeda, and Vitaflo; travel support from Amicus Therapeutics, BioMarin, Chiesi, Genzyme, Inmedica, Sobi, and Vitaflo; and has participated as a clinical trial investigator for Ultragenyx. AI has received consulting payments for and travel support to advisory boards from BioMarin. NL has received consulting payments for advisory boards from Alnylam, Amicus Therapeutics, Audentes/Astellas, BioMarin, BridgeBio/CoA Therapeutics, Chiesi/Protalix, Genzyme/Sanofi, HemoShear Therapeutics, Horizon Pharma, Jaguar Gene Therapy, Jnana Therapeutics, Leadiant Biosciences, Moderna, Nestlé Pharma, PTC Therapeutics, Recordati, Reneo, Takeda, and Ultragenyx; has received other consultancy payments from Synlogic and travel support from BioMarin; has participated as a clinical trial investigator for Aeglea, Amicus Therapeutics, Audentes/Astellas, AVROBIO, BioMarin, Chiesi/Protalix, Genzyme/Sanofi, HemoShear Therapeutics, Homology, Horizon Pharma, Moderna, Nestlé Pharma, Pfizer, PTC Therapeutics, Reneo, Synlogic, Takeda, Travere Therapeutics, and Ultragenyx; and has been Data Safety and Monitoring Chair for ACI Clinical. FM has received consulting payments from PTC Therapeutics and travel support from BioMarin. ACM has participated as a clinical trial investigator for Nutricia; has received consulting payments from Atheneum, Nestlé, and PTC Therapeutics; speaker fees/payments from AIM, Applied Pharma Research, and Nutricia; and travel support from Nutricia. ALSP has received speaker fees/payments from BioMarin. JCR has received consulting payments from Applied Pharma Research, BioMarin, Merck Serono, Nutricia, PTC Therapeutics, and Synlogic, and speaker fees/payments from Applied Pharma Research, BioMarin, Cambrooke, LifeDiet, Merck Serono, Nutricia, PIAM, and Vitaflo, as well as travel support from Applied Pharma Research, BioMarin, Glutamine, Merck Serono, PIAM, and research grants from BioMarin. FR is a managing partner of Met Ed who has received educational grants from BioMarin. SS has received speaker fees/payments from BioMarin and Sanofi. GCS is an employee of Prime Access. JS and SO were employees of Prime Access at the time the study was undertaken. Prime Access (a division of Prime, Knutsford, UK) is a company sponsored by BioMarin to conduct this study and prepare the manuscript.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
