

Efficacy and safety of a proposed omalizumab biosimilar compared to the reference product in the management of uncontrolled moderate-to-severe allergic asthma: a multicenter, phase III, randomized, double-blind, equivalency clinical trial
- PMID: 39136011
- PMCID: PMC11317399
- DOI: 10.3389/fimmu.2024.1425906
Efficacy and safety of a proposed omalizumab biosimilar compared to the reference product in the management of uncontrolled moderate-to-severe allergic asthma: a multicenter, phase III, randomized, double-blind, equivalency clinical trial
Abstract
Background and aims: Allergic asthma has a considerable burden on the quality of life. A significant portion of moderate-to-severe allergic asthma patients need omalizumab, an anti-immunoglobulin-E monoclonal antibody, as an add-on therapy. In this phase III clinical trial P043 (Zerafil®, CinnaGen, Iran) efficacy, safety, and immunogenicity were compared with Xolair® (the originator omalizumab). The primary outcome was the rate of protocol-defined asthma exacerbations.
Methods: Exacerbation rates, Asthma Control Test (ACT) results, spirometry measurements, immunogenicity, and safety were evaluated. Each subject received either medication with a dose ranging from 150 to 375 mg based on pre-treatment serum total IgE level (IU/mL) and body weight (kg) every two or four weeks for a duration of 28 weeks.
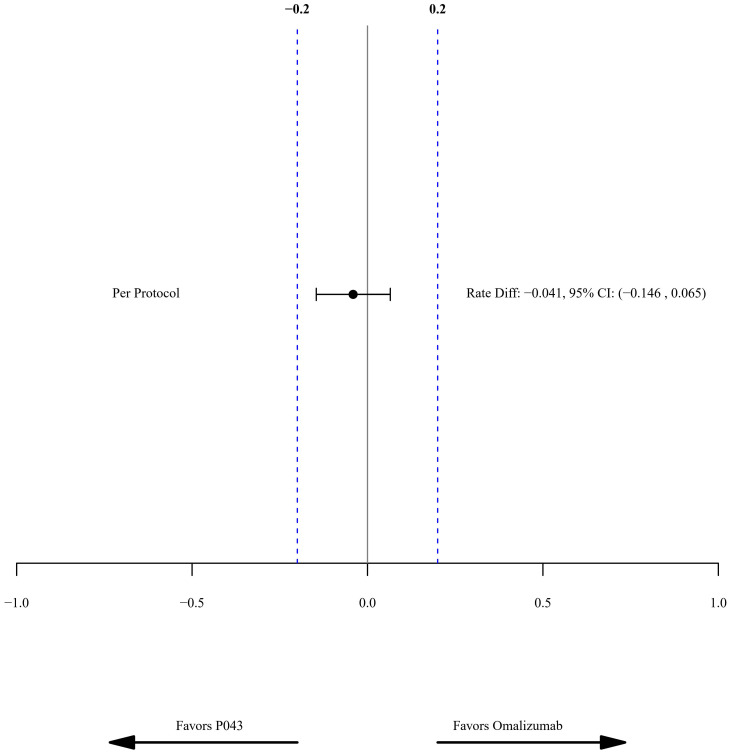
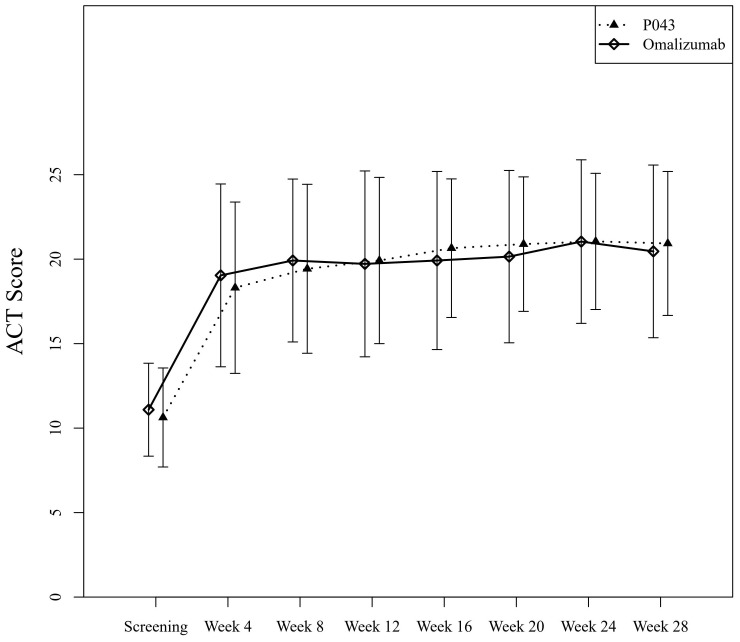
Results: Exacerbation rates were 0.150 (CI: 0.079-0.220) in the P043 group, and 0.190 (CI: 0.110-0.270) in the omalizumab group (per-protocol). The least squares mean differences of predicted Forced Expiratory Volume in the First second (FEV1) were -2.51% (CI: -7.17-2.15, P=0.29) and -3.87% (CI: -8.79-1.04, P=0.12), pre- and post-bronchodilator use. The mean ± SD of ACT scores at the screening and the last visit were 10.62 ± 2.93 and 20.93 ± 4.26 in P043 and 11.09 ± 2.75 and 20.46 ± 5.11 in the omalizumab group. A total of 288 adverse events were reported for the 256 enrolled participants. Among all, "dyspnea" and "headache" were the most reported ones. The overall incidence of adverse events (P=0.62) and serious adverse events (P=0.07) had no significant differences between the two groups. None of the samples were positive for anti-drug antibodies.
Conclusion: P043 was equivalent to omalizumab in the management of asthma in reduction of exacerbations. There was no significant difference in other efficacy and safety parameters.
Clinical trial registration: www.clinicaltrials.gov (NCT05813470) and www.IRCT.ir (IRCT20150303021315N20).
Keywords: IgE; allergic; asthma; biosimilar; omalizumab.
Copyright © 2024 Ghanei, Ghalebaghi, Sami, Torabizadeh, Mirsadraee, Amra, Tavakol, Raji, Fallahpour, Kiani, Abedini, Jabbari Azad, Mahdaviani, Attaran, Samet, Tavana, Haddadzadeh shoushtari, Nazari, AghaeiMeybodi, Fazlollahi, Ghasemi, Sabzvari, Kafi and Idani.
Conflict of interest statement
Author BG has received educational grants from AstraZeneca, Abidi, and Sanofi. Author MM has received research grants from Koushan Pharmed. Authors HR and DA have received research grants from AstraZeneca. Author MF has received research grants from Abidi. Author AK has received lecture honorarium from AstraZeneca. Author FJ has received research grants from Zist Takhmir and Vitabiotics. Author ST has received travel supports to attend scientific meetings from Novartis, GSK, and AstraZeneca. Author MH has collaborated with Jaber-ebne-hayyan. Author MRF has collaborated with Pooyesh darou. Author HK is the head of the medical department of Orchid Pharmed Company; which is in collaboration with CinnaGen company with respect to conducting clinical trials. Author AS is a member of CinnaGen medical biotechnology research center, which collaborates with universities and researchers all over the world with regards to research and development of medications and health issues. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. This study was supported by CinnaGen Company by grant number of 701/373. The sponsor also had participated in the conduction of the study.
Figures
References
-
- Asthma prevalence . Our World Data. Available online at: https://ourworldindata.org/grapher/asthma-prevalence (Accessed August 26, 2023).
-
- Asthma GI. Global strategy for asthma management and prevention; 2019. (2021) 295:. Back Cited Text.
-
- Busse WW, Massanari M, Kianifard F, Geba GP. Effect of omalizumab on the need for rescue systemic corticosteroid treatment in patients with moderate-to-severe persistent IgE-mediated allergic asthma: a pooled analysis. Curr Med Res Opin. (2007) 23:2379–86. doi: 10.1185/030079907X226258 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical