

Burden of Heart Failure in Patients With Tricuspid Regurgitation and Effect of Transcatheter Repair on Different Subdimensions of Quality of Life
- PMID: 39136306
- PMCID: PMC11963912
- DOI: 10.1161/JAHA.124.034112
Burden of Heart Failure in Patients With Tricuspid Regurgitation and Effect of Transcatheter Repair on Different Subdimensions of Quality of Life
Abstract
Background: Right-sided heart failure (HF) due to severe tricuspid regurgitation (TR) is associated with reduced quality of life (QoL). Here, we analyzed the impact of TR on specific QoL dimensions and the effect of transcatheter tricuspid valve intervention (TTVI) on individual QoL items.
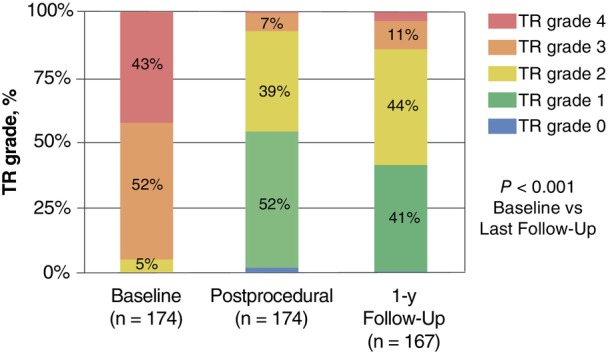
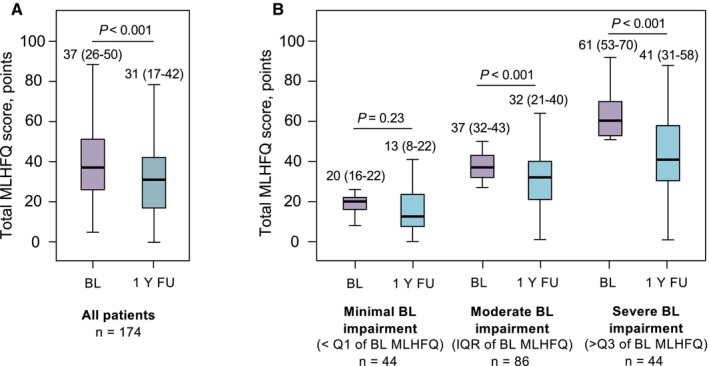
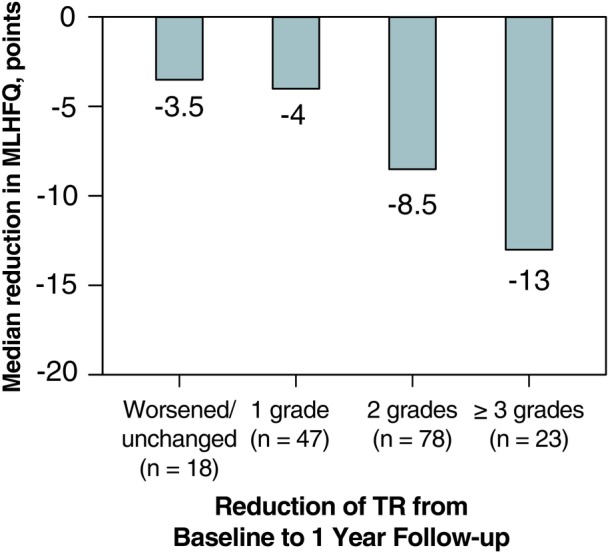
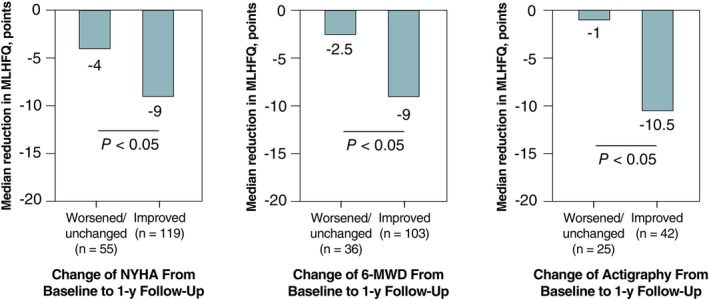
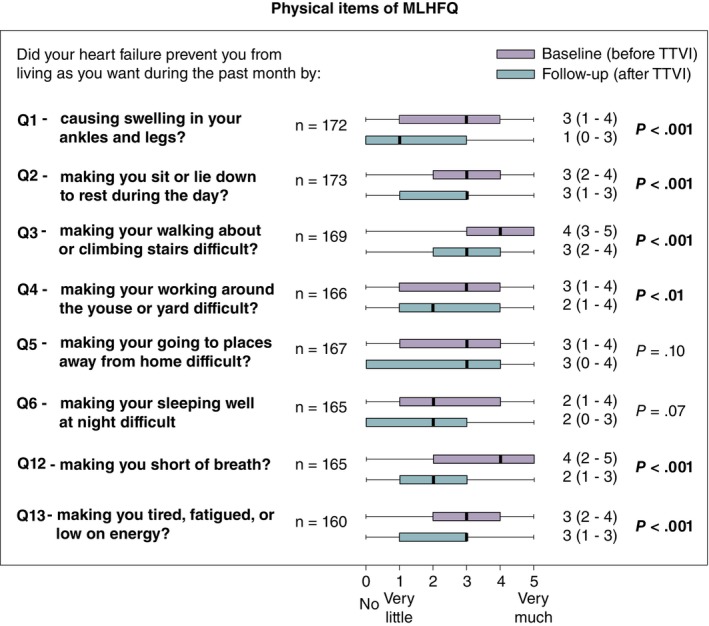
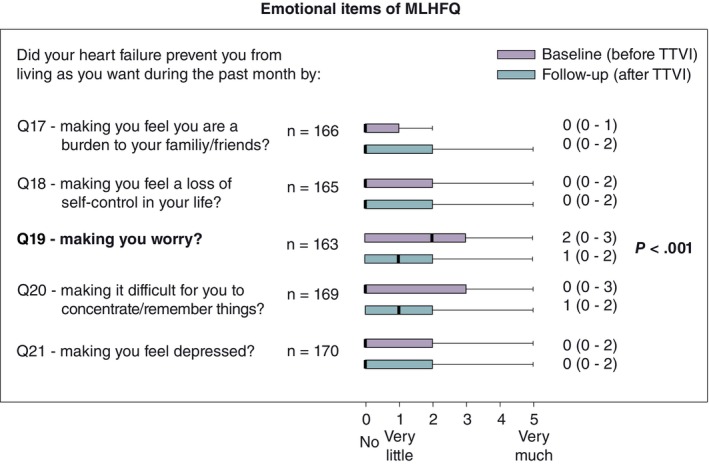
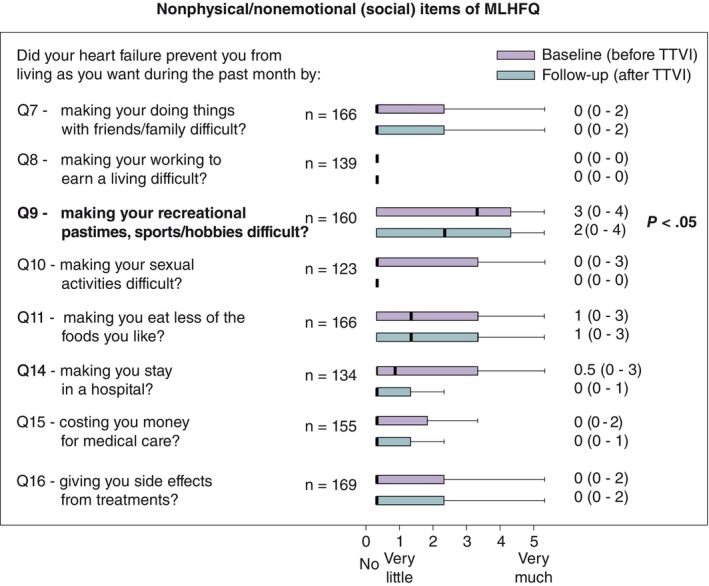
Methods and results: In this study, we included 174 patients with HF (49% women; median age, 79 years; 97% New York Heart Association ≥3) with baseline QoL assessment undergoing TTVI by transcatheter edge-to-edge-repair at our center between April 2016 and March 2022. QoL was assessed by the standardized Minnesota Living With HF Questionnaire. QoL change after TTVI and correlation to functional end points were analyzed. In addition, all QoL domains and the 21 individual items of the Minnesota Living With HF Questionnaire were analyzed. TTVI significantly reduced TR (TR ≥3: baseline 95%, 1-year-follow-up 7%; P<0.001). Total Minnesota Living with HF Questionnaire score improved from 37 (interquartile range, 26-50) points to 31 (interquartile range, 17-42) points (median follow-up-interval, 355 days; P<0.001). QoL improvement was associated with positive New York Heart Association class, 6-minute walking distance, and actigraphy changes (all P<0.05). The detailed analysis revealed that all items of the physical-related QoL dimension were impaired at baseline and strongly improved after TTVI. In contrast, the emotional and "social" Minnesota Living With HF Questionnaire dimensions were largely unaffected at baseline, yet specific items improved with TTVI.
Conclusions: In this single-center study, we delineate the QoL-associated disease burden of TR and identify specific QoL items that improved after TTVI. Our findings support TTVI in patients with reduced QoL and may add to the development of specific tools assessing the functional status of an increasing patient population undergoing TTVI.
Keywords: functional status; quality of life; right‐sided heart failure; transcatheter tricuspid edge‐to‐edge repair; transcatheter tricuspid valve intervention; tricuspid regurgitation.
Figures
Similar articles
-
Durability of benefit after transcatheter tricuspid valve intervention: insights from actigraphy.Eur J Heart Fail. 2022 Jul;24(7):1293-1301. doi: 10.1002/ejhf.2467. Epub 2022 Mar 21. Eur J Heart Fail. 2022. PMID: 35239253
-
Congestion patterns in severe tricuspid regurgitation and transcatheter treatment: Insights from a multicentre registry.Eur J Heart Fail. 2024 Apr;26(4):1004-1014. doi: 10.1002/ejhf.3235. Epub 2024 Apr 4. Eur J Heart Fail. 2024. PMID: 38571456
-
Exercise testing in patients with tricuspid regurgitation undergoing transcatheter tricuspid valve intervention.Clin Res Cardiol. 2025 Feb;114(2):261-271. doi: 10.1007/s00392-024-02554-8. Epub 2024 Oct 9. Clin Res Cardiol. 2025. PMID: 39382705 Free PMC article.
-
Transcatheter tricuspid valve intervention versus medical therapy for symptomatic tricuspid regurgitation: a meta-analysis of reconstructed time-to-event data.Int J Surg. 2024 Oct 1;110(10):6800-6809. doi: 10.1097/JS9.0000000000001773. Int J Surg. 2024. PMID: 39705669 Free PMC article.
-
Transcatheter Interventions for Tricuspid Valve Disease: What to Do and Who to Do It On.Can J Cardiol. 2021 Jul;37(7):953-967. doi: 10.1016/j.cjca.2020.12.029. Epub 2021 Jan 22. Can J Cardiol. 2021. PMID: 33493660 Review.
Cited by
-
Quality of life after transcatheter tricuspid valve repair: results from the Tri.FR trial.ESC Heart Fail. 2025 Aug;12(4):3053-3061. doi: 10.1002/ehf2.15327. Epub 2025 May 19. ESC Heart Fail. 2025. PMID: 40387042 Free PMC article. Clinical Trial.
-
Omentin-1 as a promising biomarker and therapeutic target in hypertension and heart failure: a comprehensive review.Naunyn Schmiedebergs Arch Pharmacol. 2025 Mar 24. doi: 10.1007/s00210-025-04008-y. Online ahead of print. Naunyn Schmiedebergs Arch Pharmacol. 2025. PMID: 40126671 Review.
References
-
- Neuhold S, Huelsmann M, Pernicka E, Graf A, Bonderman D, Adlbrecht C, Binder T, Maurer G, Pacher R, Mascherbauer J. Impact of tricuspid regurgitation on survival in patients with chronic heart failure: unexpected findings of a long‐term observational study. Eur Heart J. 2013;34:844–852. doi: 10.1093/eurheartj/ehs465 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
