EHMT1/2 Inhibition Promotes Regression of Therapy-Resistant Ovarian Cancer Tumors in a CD8 T-cell-Dependent Manner
- PMID: 39136655
- PMCID: PMC11614706
- DOI: 10.1158/1541-7786.MCR-24-0067
EHMT1/2 Inhibition Promotes Regression of Therapy-Resistant Ovarian Cancer Tumors in a CD8 T-cell-Dependent Manner
Abstract
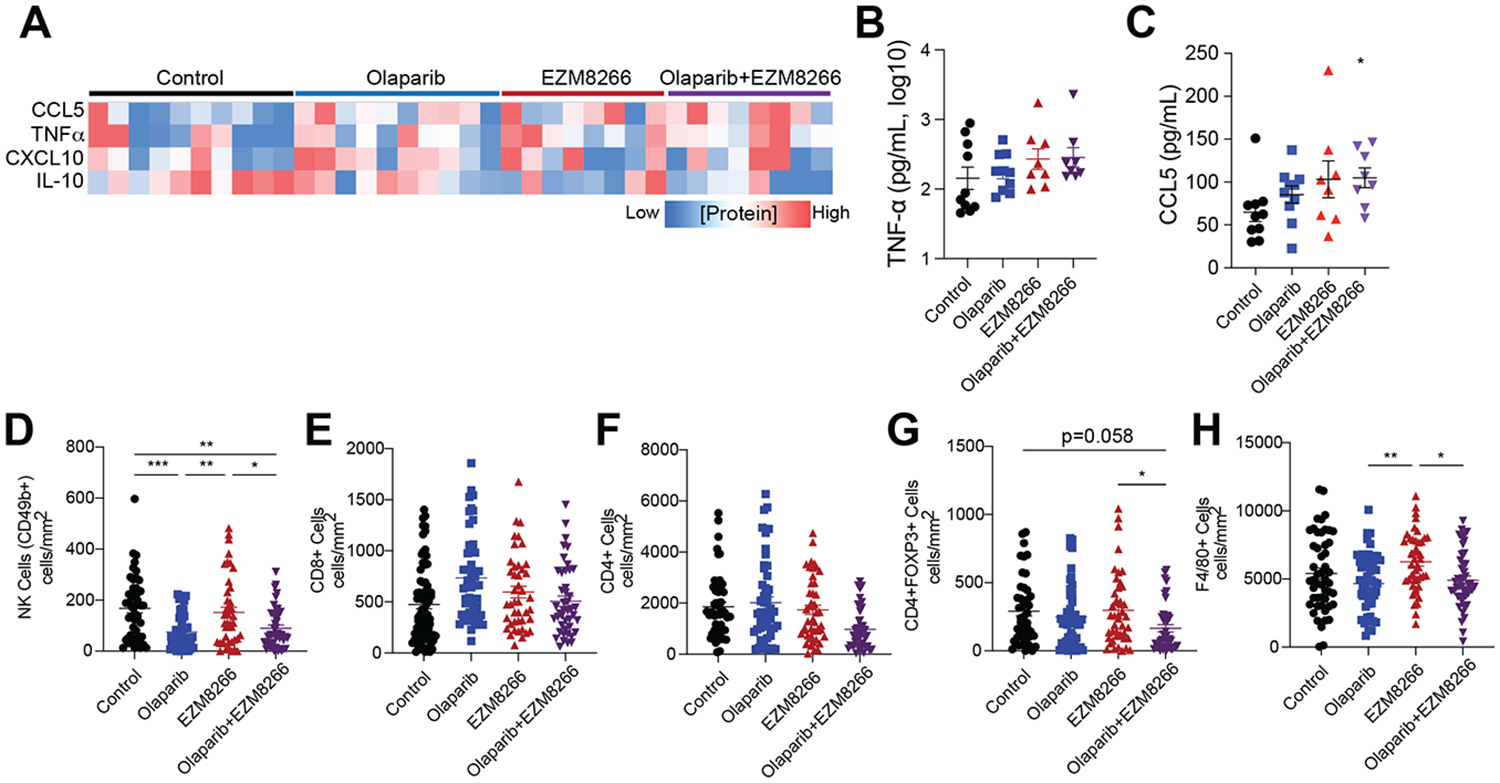
Poly ADP-ribose polymerase inhibitors (PARPi) are first-line maintenance therapy for ovarian cancer and an alternative therapy for several other cancer types. However, PARPi-resistance is rising, and there is currently an unmet need to combat PARPi-resistant tumors. Here, we created an immunocompetent, PARPi-resistant mouse model to test the efficacy of combinatory PARPi and euchromatic histone methyltransferase 1/2 inhibitor (EHMTi) in the treatment of PARPi-resistant ovarian cancer. We discovered that inhibition of EHMT1/2 resensitizes cells to PARPi. Markedly, we show that single EHMTi and combinatory EHMTi/PARPi significantly reduced PARPi-resistant tumor burden and that this reduction is partially dependent on CD8 T cells. Altogether, our results show a low-toxicity drug that effectively treats PARPi-resistant ovarian cancer in an immune-dependent manner, supporting its entry into clinical development and potential incorporation of immunotherapy. Implications: Targeting the epigenome of therapy-resistant ovarian cancer induces an antitumor response mediated in part through an antitumor immune response.
©2024 American Association for Cancer Research.
Conflict of interest statement
Conflict of interest statement: The authors declare no potential conflicts of interest.
Figures




References
-
- Kuroki L, Guntupalli SR. Treatment of epithelial ovarian cancer. BMJ. British Medical Journal Publishing Group; 2020;371:m3773. - PubMed
-
- Moore K, Colombo N, Scambia G, Kim B-G, Oaknin A, Friedlander M, et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N Engl J Med. 2018;379:2495–505. - PubMed
-
- Wu L, Zhu J, Yin R, Wu X, Lou G, Wang J, et al. Olaparib maintenance therapy in patients with newly diagnosed advanced ovarian cancer and a BRCA1 and/or BRCA2 mutation: SOLO1 China cohort. Gynecologic Oncology [Internet]. 2020. [cited 2020 Nov 30]; Available from: http://www.sciencedirect.com/science/article/pii/S0090825820340130 - PubMed
-
- Mirza MR, Monk BJ, Herrstedt J, Oza AM, Mahner S, Redondo A, et al. Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer. N Engl J Med. 2016;375:2154–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 CA285446/CA/NCI NIH HHS/United States
- R00 CA194318/CA/NCI NIH HHS/United States
- R35 GM143108/GM/NIGMS NIH HHS/United States
- OC170228/U.S. Department of Defense (DOD)
- P30 CA046934/CA/NCI NIH HHS/United States
- R03 CA249571/CA/NCI NIH HHS/United States
- RSG-19-129-01-DDC/American Cancer Society (ACS)
- R37 CA261987/CA/NCI NIH HHS/United States
- R01CA266100/All of Us Research Program (All of Us NIH)
- R37CA261987/All of Us Research Program (All of Us NIH)
- R35 GM128822/GM/NIGMS NIH HHS/United States
- R01 CA266100/CA/NCI NIH HHS/United States
- R35GM128822/All of Us Research Program (All of Us NIH)
- P30CA046934/All of Us Research Program (All of Us NIH)
- OC200302/US Department of Defense
- OC200225/US Department of Defense
- OC210257/US Department of Defense
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials