

Patient Factors Influencing Outcomes at 12-Year Follow-up of Hip Arthroscopy for Femoroacetabular Impingement
- PMID: 39137412
- PMCID: PMC11344956
- DOI: 10.1177/03635465241265721
Patient Factors Influencing Outcomes at 12-Year Follow-up of Hip Arthroscopy for Femoroacetabular Impingement
Abstract
Background: Arthroscopic treatment of femoroacetabular impingement has increased in popularity since the early 2000s when it was first described, although only a few midterm follow-up studies have been published.
Purpose: To describe the outcomes of patients undergoing hip arthroscopy for femoroacetabular impingement at a mean 12-year follow-up and to determine the risk factors for failure.
Study design: Case-control study; Level of evidence, 3.
Methods: The Non-Arthritic Hip Score (NAHS) and a radiographic evaluation were completed preoperatively and at midterm follow-up. Participants were divided into 2 groups according to their clinical evolution. The success group consisted of patients whose NAHS at the final follow-up was above the established Patient Acceptable Symptom State (PASS) threshold of 81.9, whereas patients who underwent a second surgical intervention or did not reach the PASS threshold at final follow-up were assigned to the failure group. These groups were compared to identify preoperative differences in demographic, pathological, and surgical factors.
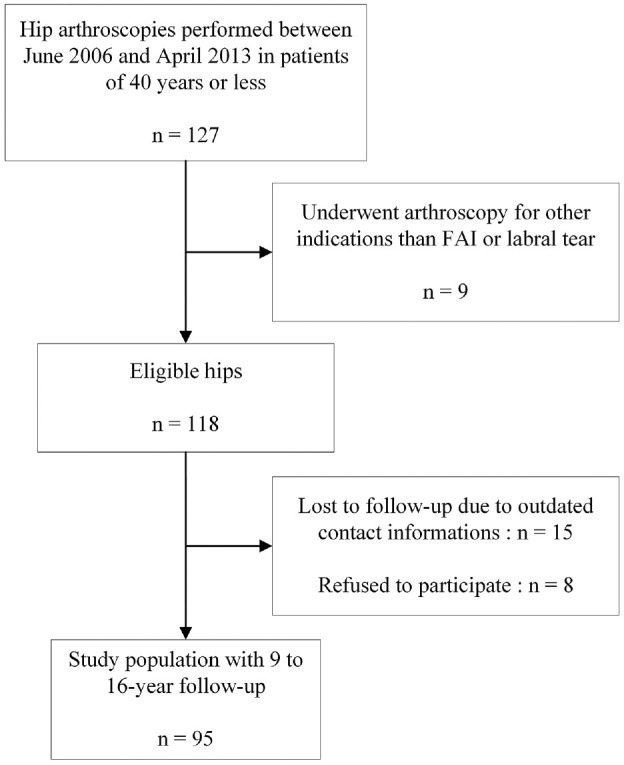
Results: A total of 95 hips were included, after 23 were lost to follow-up (80.5% follow-up). At a mean follow-up of 12.1 years (range, 9.2-16.0 years), 9 hips required total hip arthroplasty (9.5%), 5 required revision hip arthroscopy (5.3%), 29 did not achieve the NAHS PASS threshold (30.5%), and 52 achieved the NAHS PASS threshold (54.7%). The mean NAHS was 82.4 at final follow-up compared with 66.9 preoperatively (mean difference = 15.5; P < .001). Higher mean body mass index (24.9 vs 23.0; P = .030), older age (30.0 vs 27.2; P = .035), and inferior preoperative lateral joint space width (3.9 vs 4.4; P = .019) were associated with inferior prognosis in the failure group versus success group. Osteoarthritis progression was observed in 69.2% of the failure group and in 34.8% of the success group (P = .082). Labral ossification was observed in 78.3% of all patients, and its lateral projection length was statistically associated with failure (P = .015).
Conclusion: At a mean 12-year follow-up, hip arthroscopy for femoroacetabular impingement led to significant clinical improvement, with 55% PASS achievement. In total, 31% of patients were below the PASS threshold, 5% had revision arthroscopy, and only 9% had conversion to total hip arthroplasty for a 45% global failure rate. Increased body mass index, older age, and smaller preoperative lateral joint space width were significant negative prognostic factors. Postoperative degenerative changes were highly prevalent and demonstrated association with failure.
Keywords: femoroacetabular impingement; hip arthroscopy; labral repair; osteoarthritis.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D. has received research support from SOFCOT. B.A.M. has received speaking fees from Arthrex and Pendopharm. E.L.B. is on the advisory board of Pendopharm and Bodycad; has received speaking fees from Pendopharm, Sanofi, Stryker, Smith + Nephew, and ConMed; and has received royalties from Bodycad. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures

References
-
- Bech NH, Sierevelt IN, de Waard S, Joling BSH, Kerkhoffs G, Haverkamp D. Capsular closure versus unrepaired interportal capsulotomy after hip arthroscopy in patients with femoroacetabular impingement: results of a patient-blinded randomised controlled trial. Hip Int. 2023;33(1):94-101. doi: 10.1177/11207000211005762 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
