

Simultaneous prognostic score validation in patients with out-of-hospital cardiac arrest by a post-hoc analysis based on national multicenter registry
- PMID: 39138314
- PMCID: PMC11322376
- DOI: 10.1038/s41598-024-69815-4
Simultaneous prognostic score validation in patients with out-of-hospital cardiac arrest by a post-hoc analysis based on national multicenter registry
Abstract
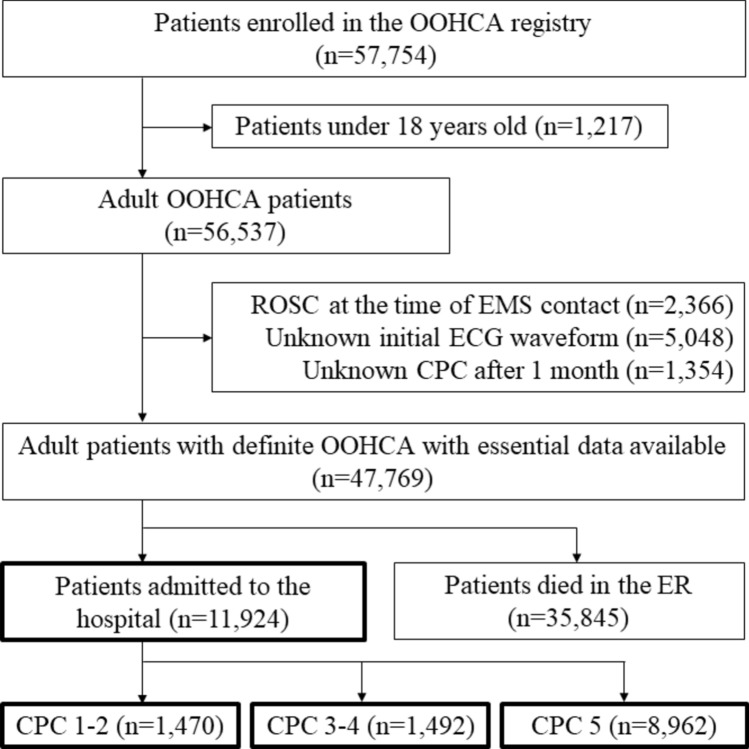
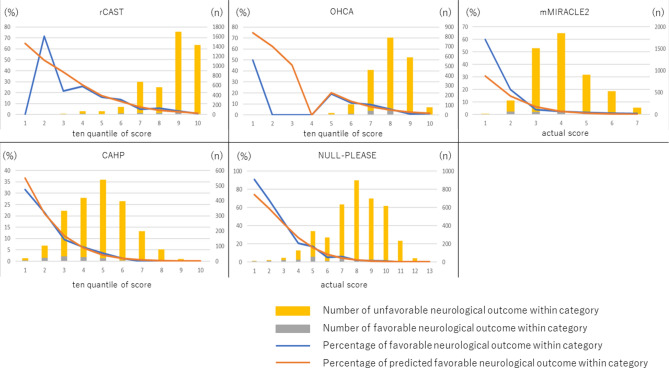
Using a nationwide multicenter prospective registry in Japan's data, we calculated prognostic and predictive scores, including the Out-of-Hospital Cardiac Arrest (OHCA); Cardiac Arrest Hospital Prognosis (CAHP); Nonshockable rhythm, Unwitnessed arrest, Long no-flow or Long low-flow period, blood PH < 7.2, Lactate > 7.0 mmol/L, End-stage chronic kidney disease on dialysis, Age ≥ 85 years, Still resuscitation, and Extracardiac cause (NULL-PLEASE); revised post-Cardiac Arrest Syndrome for Therapeutic hypothermia (rCAST); and MIRACLE2 scores, for adult patients with cardiac arrest. The MIRACLE2 score was validated with the modified MIRACLE2 score, which excludes information of pupillary reflexes. Each score was calculated only for the cases with no missing data for the variables used. These scores' accuracies were compared using neurological outcomes 30 days after out-of-hospital cardiac arrest (OOHCA). Patients with a cerebral performance category scale of 1 or 2 were designated as having favorable neurological outcomes. Each score's discrimination ability was evaluated by the receiver operating characteristic curve's area under the curve (AUC). To assess in detail in areas of high specificity and high sensitivity, which are areas of interest to clinicians, partial AUCs were also used. The analysis included 11,924 hospitalized adult patients. The AUCs of the OHCA, MIRACLE2, CAHP, rCAST, and NULL-PLEASE scores for favorable neurological outcomes were 0.713, 0.727, 0.785, 0.761, and 0.831, respectively. The CAHP and NULL-PLEASE scores were significantly more accurate than the rest. Accuracies did not differ significantly between the CAHP and NULL-PLEASE scores. The NULL-PLEASE score was significantly better at discriminating favorable neurological prognoses at 30 days in patients with OOHCA compared to other scoring systems.
© 2024. The Author(s).
Conflict of interest statement
Kota Ono received a consulting fee for statistical analysis from the department of emergency medicine, Hokkaido university hospital, and Kota Ono is also an employee of AbbVie GK. All other authors do not have any competing interest or conflicts of interest.
Figures

Similar articles
-
Simultaneous external validation of various cardiac arrest prognostic scores: a single-center retrospective study.Scand J Trauma Resusc Emerg Med. 2021 Aug 14;29(1):117. doi: 10.1186/s13049-021-00935-w. Scand J Trauma Resusc Emerg Med. 2021. PMID: 34391466 Free PMC article.
-
Prediction of the neurological outcomes post-cardiac arrest: A prospective validation of the CAST and rCAST.Am J Emerg Med. 2024 Jan;75:46-52. doi: 10.1016/j.ajem.2023.10.028. Epub 2023 Oct 20. Am J Emerg Med. 2024. PMID: 38149972
-
External validation of cardiac arrest-specific prognostication scores developed for early prognosis estimation after out-of-hospital cardiac arrest in a Korean multicenter cohort.PLoS One. 2022 Apr 1;17(4):e0265275. doi: 10.1371/journal.pone.0265275. eCollection 2022. PLoS One. 2022. PMID: 35363794 Free PMC article.
-
Prediction performance of scoring systems after out-of-hospital cardiac arrest: A systematic review and meta-analysis.PLoS One. 2024 Feb 1;19(2):e0293704. doi: 10.1371/journal.pone.0293704. eCollection 2024. PLoS One. 2024. PMID: 38300929 Free PMC article.
-
Out-of-hospital cardiac arrest: A systematic review of current risk scores to predict survival.Am Heart J. 2021 Apr;234:31-41. doi: 10.1016/j.ahj.2020.12.011. Epub 2020 Dec 31. Am Heart J. 2021. PMID: 33387469
References
-
- Al-Khatib, S. M. et al. AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Executive summary: A report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart rhythm society. J. Am. Coll. Cardiol.72, 1677–1749 (2018). 10.1016/j.jacc.2017.10.053 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
