

Clinical application of whole-genome sequencing of solid tumors for precision oncology
- PMID: 39138315
- PMCID: PMC11371929
- DOI: 10.1038/s12276-024-01288-x
Clinical application of whole-genome sequencing of solid tumors for precision oncology
Abstract
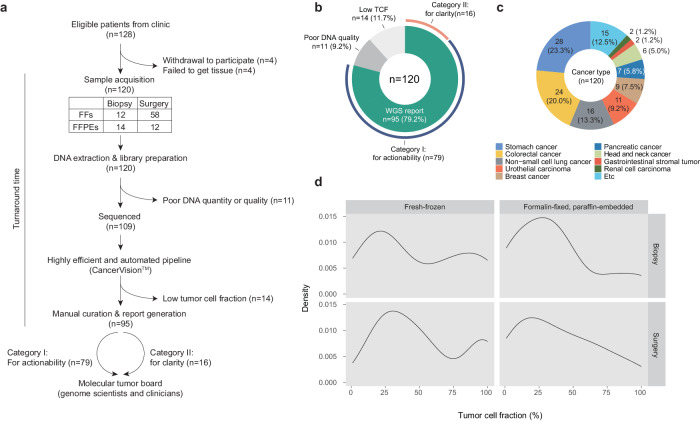
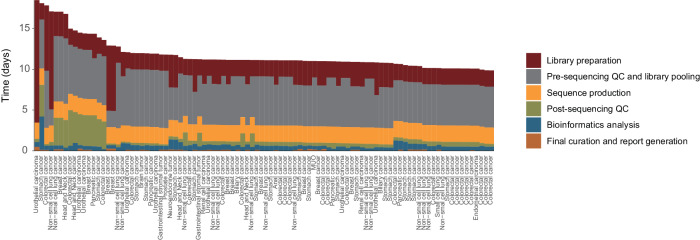
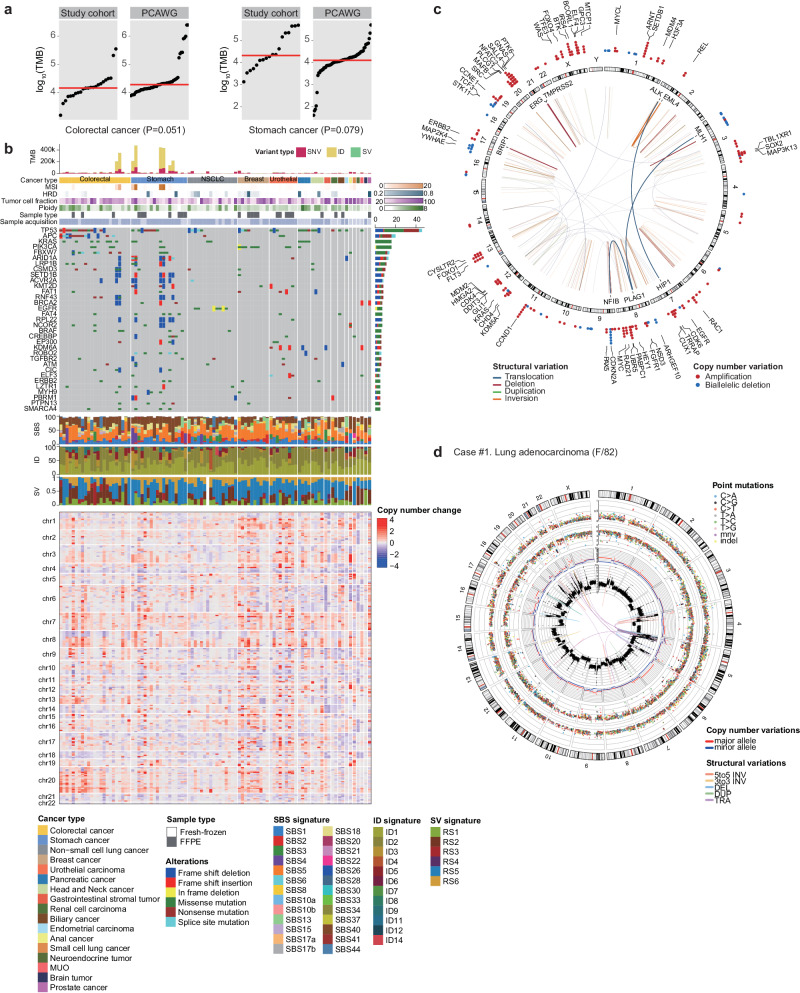
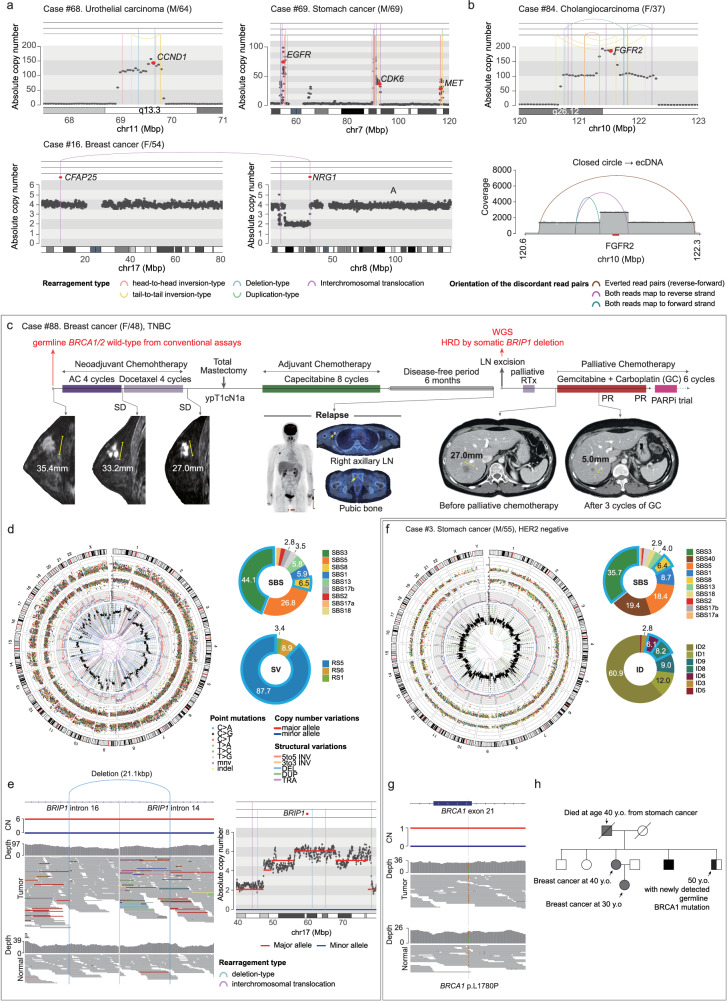
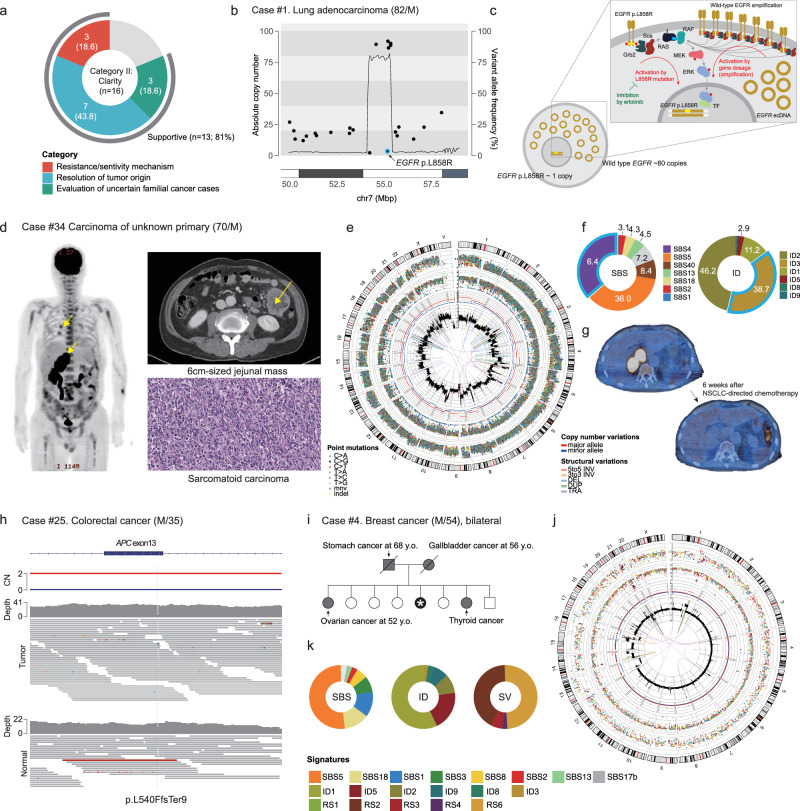
Genomic alterations in tumors play a pivotal role in determining their clinical trajectory and responsiveness to treatment. Targeted panel sequencing (TPS) has served as a key clinical tool over the past decade, but advancements in sequencing costs and bioinformatics have now made whole-genome sequencing (WGS) a feasible single-assay approach for almost all cancer genomes in clinical settings. This paper reports on the findings of a prospective, single-center study exploring the real-world clinical utility of WGS (tumor and matched normal tissues) and has two primary objectives: (1) assessing actionability for therapeutic options and (2) providing clarity for clinical questions. Of the 120 patients with various solid cancers who were enrolled, 95 (79%) successfully received genomic reports within a median of 11 working days from sampling to reporting. Analysis of these 95 WGS reports revealed that 72% (68/95) yielded clinically relevant insights, with 69% (55/79) pertaining to therapeutic actionability and 81% (13/16) pertaining to clinical clarity. These benefits include the selection of informed therapeutics and/or active clinical trials based on the identification of driver mutations, tumor mutational burden (TMB) and mutational signatures, pathogenic germline variants that warrant genetic counseling, and information helpful for inferring cancer origin. Our findings highlight the potential of WGS as a comprehensive tool in precision oncology and suggests that it should be integrated into routine clinical practice to provide a complete image of the genomic landscape to enable tailored cancer management.
© 2024. The Author(s).
Conflict of interest statement
R.K., B.B.L.O., E.J., Si.L., J.Y.S., J.-Y.Y., J.P., K.Y., Y.K., W.-C.L., H.P., J.L., B.Y., J.K., J.-Y.K., Sa.L., Y.L., and B.-R.L. are employees of Inocras, Inc.. Y.S.J. is a cofounder, member of the board of trustees, and shareholder of Inocras, Inc. M.K. has received research grants from Inocras and Genome and Company. However, this commercial affiliation did not have any role in the data collection and analysis. These coauthors contributed with study design, decision to publish, and preparation of the manuscript. All the other authors declare no conflicts of interest in the authorship or publication of this contribution.
Figures

References
-
- ICGC/TCGA Pan-Cancer Analysis of Whole Genomes Consortium. Pan-cancer analysis of whole genomes. Nature578, 82–93 (2020).
-
- Garraway, L. A. & Lander, E. S. Lessons from the cancer genome. Cell153, 17–37 (2013). - PubMed
-
- Slamon, D. J. et al. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science235, 177–182 (1987). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
