

Distinctive evolution of alveolar T cell responses is associated with clinical outcomes in unvaccinated patients with SARS-CoV-2 pneumonia
- PMID: 39138384
- PMCID: PMC11490290
- DOI: 10.1038/s41590-024-01914-w
Distinctive evolution of alveolar T cell responses is associated with clinical outcomes in unvaccinated patients with SARS-CoV-2 pneumonia
Abstract
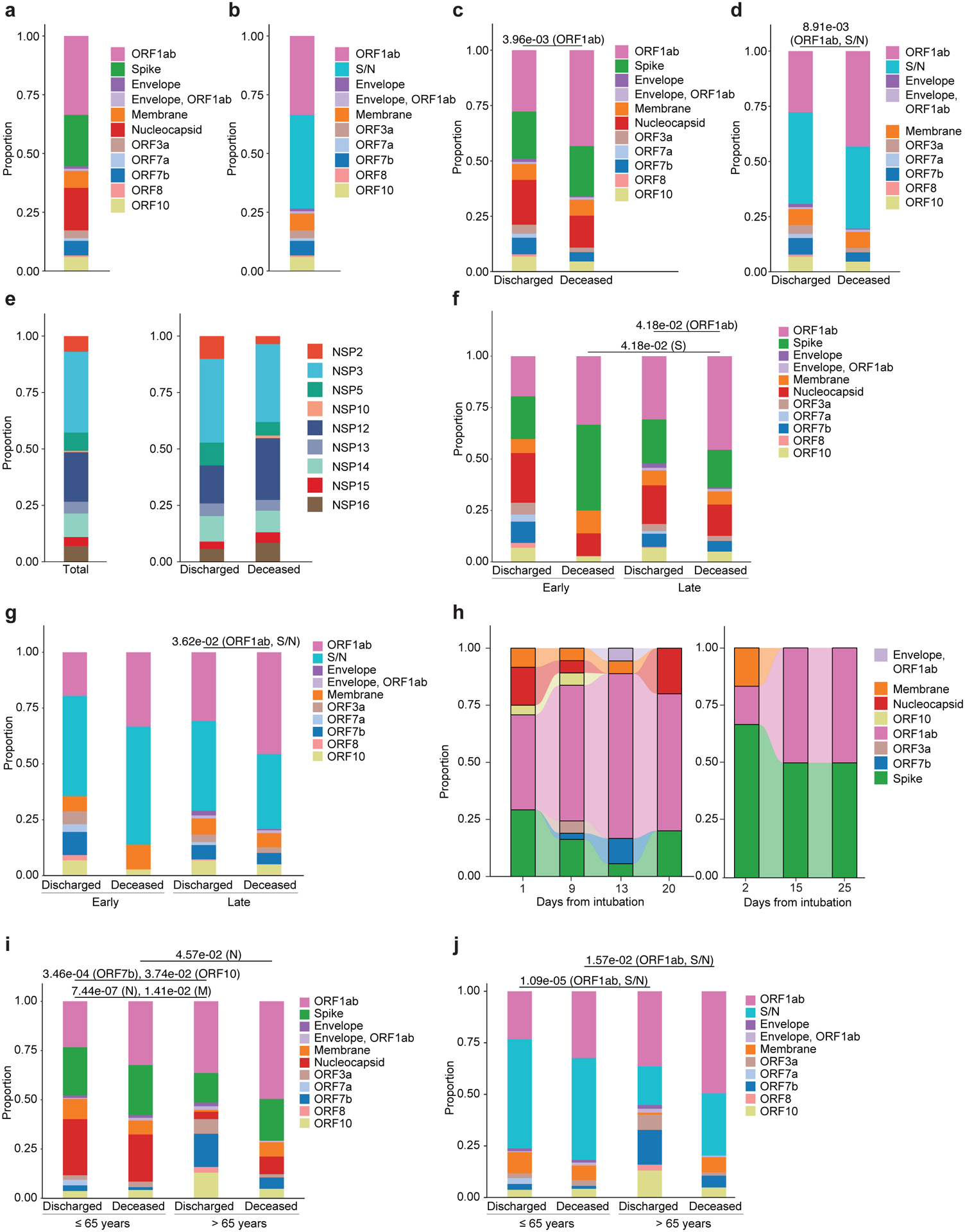
The evolution of T cell molecular signatures in the distal lung of patients with severe pneumonia is understudied. Here, we analyzed T cell subsets in longitudinal bronchoalveolar lavage fluid samples from 273 patients with severe pneumonia, including unvaccinated patients infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) or with respiratory failure not linked to pneumonia. In patients with SARS-CoV-2 pneumonia, activation of interferon signaling pathways, low activation of the NF-κB pathway and preferential targeting of spike and nucleocapsid proteins early after intubation were associated with favorable outcomes, whereas loss of interferon signaling, activation of NF-κB-driven programs and specificity for the ORF1ab complex late in disease were associated with mortality. These results suggest that in patients with severe SARS-CoV-2 pneumonia, alveolar T cell interferon responses targeting structural SARS-CoV-2 proteins characterize individuals who recover, whereas responses against nonstructural proteins and activation of NF-κB are associated with poor outcomes.
© 2024. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
Competing Interest Statement
BDS holds United States Patent No. US 10,905,706 B2, “Compositions and Methods to Accelerate Resolution of Acute Lung Inflammation”, and serves on the Scientific Advisory Board of Zoe Biosciences, outside of the submitted work. The other authors have no competing interests to declare.
Figures














Update of
-
A distinctive evolution of alveolar T cell responses is associated with clinical outcomes in unvaccinated patients with SARS-CoV-2 pneumonia.bioRxiv [Preprint]. 2023 Dec 14:2023.12.13.571479. doi: 10.1101/2023.12.13.571479. bioRxiv. 2023. Update in: Nat Immunol. 2024 Sep;25(9):1607-1622. doi: 10.1038/s41590-024-01914-w. PMID: 38168346 Free PMC article. Updated. Preprint.
References
-
- Markov NS et al. SCRIPT CarpeDiem Dataset: demographics, outcomes, and per-day clinical parameters for critically ill patients with suspected pneumonia (version 1.1.0). PhysioNet; 2023.
Methods References
MeSH terms
Substances
Grants and funding
- R01 HL153122/HL/NHLBI NIH HHS/United States
- S10 OD032243/OD/NIH HHS/United States
- R21 AG075423/AG/NIA NIH HHS/United States
- K23 HL169815/HL/NHLBI NIH HHS/United States
- R01 HL094643/HL/NHLBI NIH HHS/United States
- P01 HL154998/HL/NHLBI NIH HHS/United States
- U01 TR003528/TR/NCATS NIH HHS/United States
- R01 AI177498/AI/NIAID NIH HHS/United States
- R01 LM013337/LM/NLM NIH HHS/United States
- R01 HL147290/HL/NHLBI NIH HHS/United States
- R01 HL147575/HL/NHLBI NIH HHS/United States
- R01 HL134800/HL/NHLBI NIH HHS/United States
- T32 HL076139/HL/NHLBI NIH HHS/United States
- I01 CX001777/CX/CSRD VA/United States
- R01 ES034350/ES/NIEHS NIH HHS/United States
- U19 AI181102/AI/NIAID NIH HHS/United States
- F32 HL162377/HL/NHLBI NIH HHS/United States
- P01 AG049665/AG/NIA NIH HHS/United States
- 24PRE1196998/AHA/American Heart Association-American Stroke Association/United States
- T32 AI007476/AI/NIAID NIH HHS/United States
- U19 AI135964/AI/NIAID NIH HHS/United States
- R01 HL153312/HL/NHLBI NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- T32 AG020506/AG/NIA NIH HHS/United States
- R01 HL158139/HL/NHLBI NIH HHS/United States
- P30 CA060553/CA/NCI NIH HHS/United States
- U19AI135964/U.S. Department of Health & Human Services | NIH | National Institute of Allergy and Infectious Diseases (NIAID)
- F31 AG071225/AG/NIA NIH HHS/United States
- R01 HL149883/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
