

Prosopagnosia is highly comorbid in individuals with probable developmental coordination disorder
- PMID: 39138399
- PMCID: PMC12267868
- DOI: 10.1177/17470218241275977
Prosopagnosia is highly comorbid in individuals with probable developmental coordination disorder
Abstract
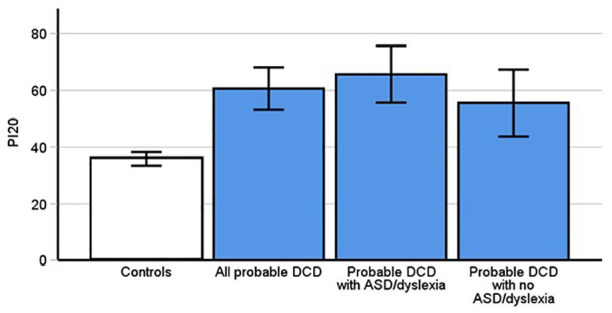
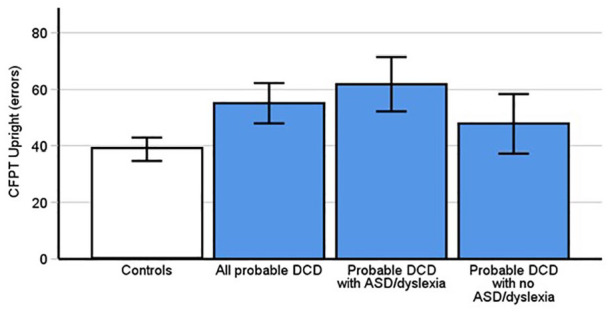
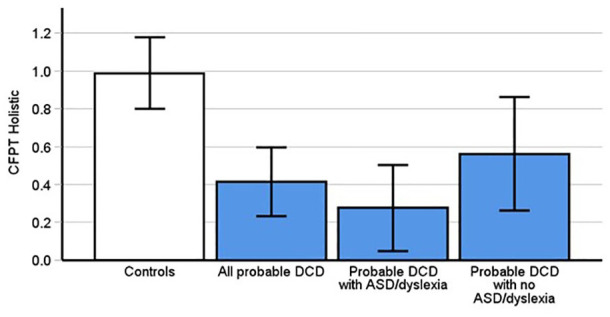
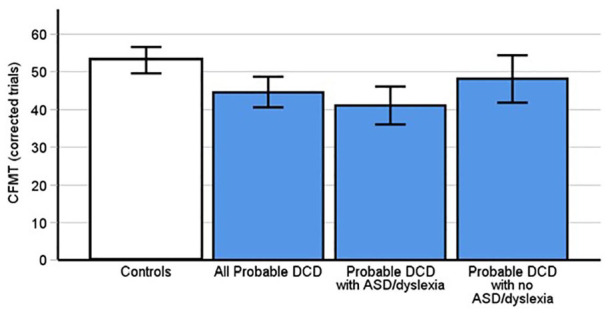
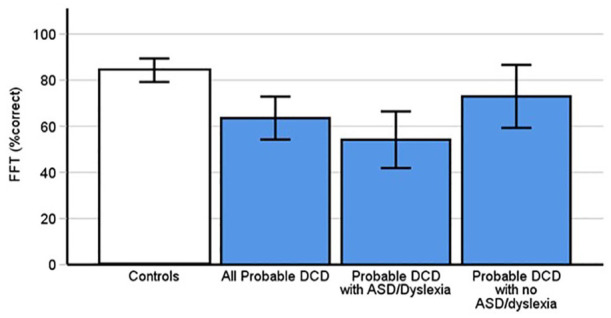
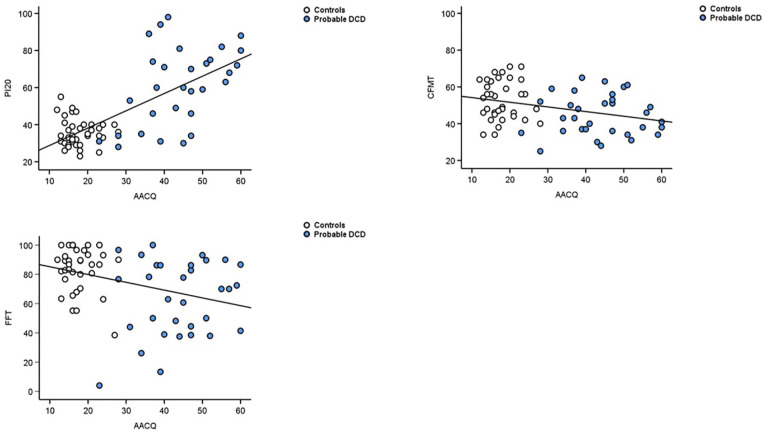
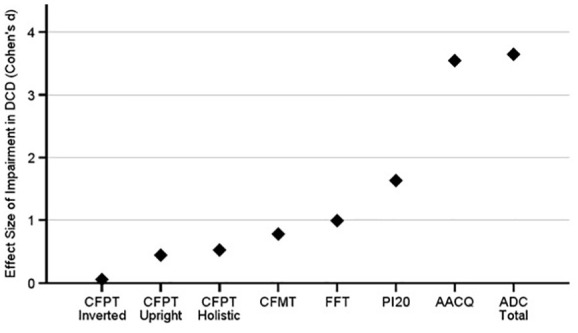
Developmental co-ordination disorder (DCD) is characterised by difficulties in motor control and coordination from early childhood. While problems processing facial identity are often associated with neurodevelopmental conditions, such issues have never been directly tested in adults with DCD. We tested this possibility through a range of tasks and assessed the prevalence of developmental prosopagnosia (i.e. lifelong difficulties with faces), in a group comprising individuals who self-reported a diagnosis of, or suspected that they had, DCD. Strikingly, we found 56% of this probable DCD group met recently recommended criteria for a diagnosis of prosopagnosia, with 22% acquiring a diagnosis using traditional cognitive task-based methods. Moreover, their problems with faces were apparent on both unfamiliar and familiar face memory tests, as well as on a facial perception task (i.e. could they tell faces apart). Positive correlations were found between self-report measures assessing movement and coordination problems, and objective difficulties on experimental face identity processing tasks, suggesting widespread neurocognitive disruption in DCD. Importantly, some issues in identity processing in our probable DCD group remained even after excluding participants with comorbid conditions traditionally associated with difficulties in face recognition, that is, autism and dyslexia. We recommend that any diagnostic test for DCD should include an assessment for prosopagnosia. Given the high prevalence of prosopagnosia in our probable DCD group, and the positive correlations between DCD and prosopagnosia symptoms, there may be a stronger link between movement and facial identity abilities than previously thought.
Keywords: DCD; developmental coordination disorder; dyspraxia; face perception; face recognition; motor; prosopagnosia.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Åsberg Johnels J., Hadjikhani N., Sundqvist M., Galazka M. A. (2022). Face processing in school children with dyslexia: Neuropsychological and eye-tracking findings. Developmental Neuropsychology, 47(2), 78–92. - PubMed
-
- American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). American Psychiatric Publishing.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
