

Treating acid reflux without compressing the food passageway: 4-year safety and clinical outcomes with the RefluxStop device in a prospective multicenter study
- PMID: 39138680
- PMCID: PMC11458627
- DOI: 10.1007/s00464-024-11114-0
Treating acid reflux without compressing the food passageway: 4-year safety and clinical outcomes with the RefluxStop device in a prospective multicenter study
Abstract
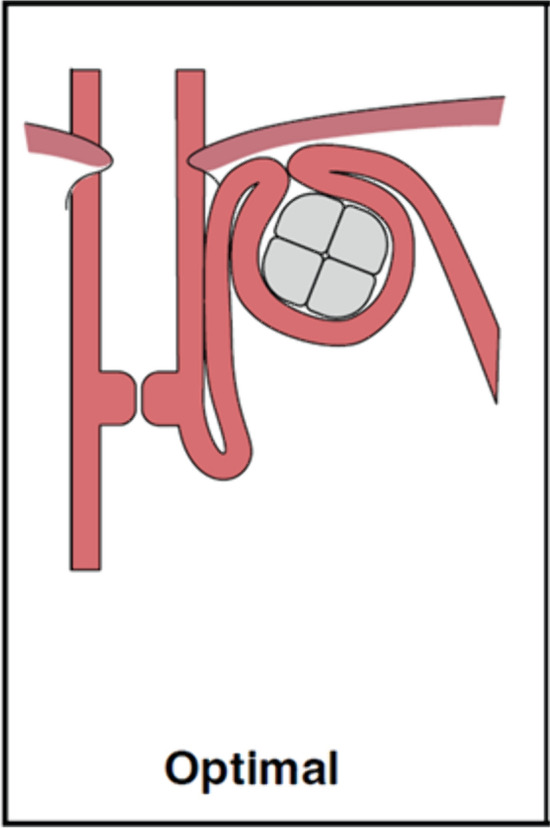
Introduction: RefluxStop is an implantable device for laparoscopic surgical treatment of gastroesophageal reflux disease (GERD) to restore and maintain lower esophageal sphincter and angle of His anatomy without encircling and putting pressure on the food passageway, thereby avoiding side effects such as dysphagia and bloating seen with traditional fundoplication. This study reports the clinical outcomes with RefluxStop at 4 years following implantation of the device.
Methods: A prospective, single arm, multicenter clinical investigation analyzing safety and effectiveness of the RefluxStop device in 50 patients with chronic GERD.
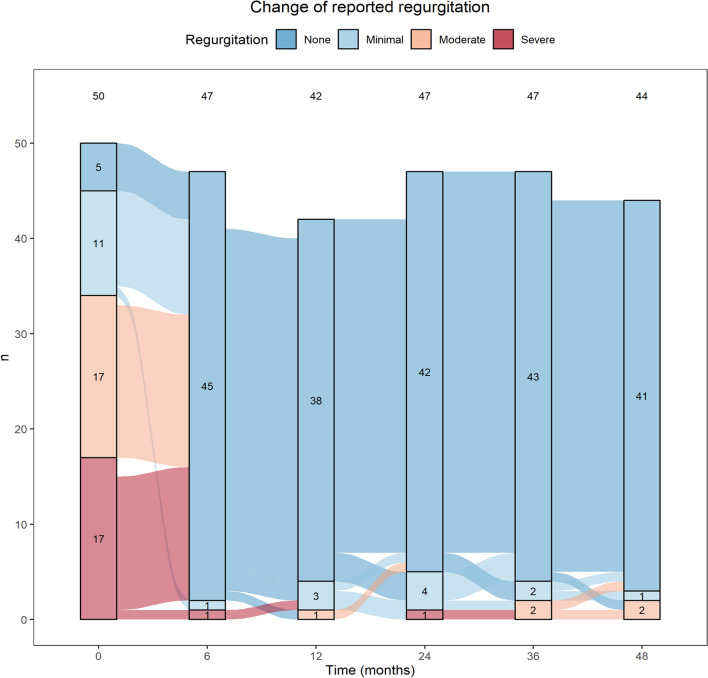
Results: Available data are presented for 44 patients at 4 years with the addition of three patients at 3 years carried forward. At 4 years, median GERD-HRQL score was 90% reduced compared to baseline. Two patients (2/44) used regular daily proton pump inhibitors (PPIs) despite subsequent 24-h pH monitoring off PPI therapy yielding normal results. There were no device-related adverse events (AEs), esophageal dilations, migrations, or explants during the entire study period. AEs reported between 1 and 4 years were as follows: one subject with heartburn and a pathologic pH result with device positioned too low at surgery; one subject with dysphagia, thus, 46/47 patients reported no dysphagia-related AEs between years 1 and 4. Two patients (2/47) were dissatisfied with treatment despite normal 24-h pH monitoring, of whom one had manometry-verified dysmotility at 6 months, indicating dissatisfaction for reasons other than acid reflux.
Conclusion: These results confirm the excellent and already published 1-year results as stable in the long-term, supporting the safety and effectiveness of the RefluxStop device in treating GERD for over 4 years. GERD-HRQL score, pH testing, and PPI usage indicate treatment success without dysphagia or gas-bloating and only minimal incidence of other AEs. This favorably low rate of AEs is likely attributable to RefluxStop's dynamic physiologic interaction and non-encircling nature.
Keywords: Dysphagia; Gas-bloating; Gastroesophageal reflux disease (GERD); RefluxStop; Surgery; pH monitoring.
© 2024. The Author(s).
Conflict of interest statement
Authors László Harsányi, Zsolt Kincses and Áron Altorjay declare that they have no competing interests. Joerg Zehetner has received honoraria from Implantica and Johnson & Johnson and grants/contracts from Implantica and Johnson & Johnson, not in relation to the present manuscript.
Figures
References
-
- Kamolz T, Pointner R, Velanovich V (2003) The impact of gastroesophageal reflux disease on quality of life. Surg Endosc 17(8):1193–1199. 10.1007/s00464-002-9229-4 - PubMed
-
- Ho ALK, Smyth EC (2020) A global perspective on oesophageal cancer: two diseases in one. Lancet Gastroenterol Hepatol 5(6):521–522. 10.1016/s2468-1253(20)30047-9 - PubMed
-
- Lagergren J, Bergström R, Lindgren A, Nyrén O (1999) Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 340(11):825–831. 10.1056/nejm199903183401101 - PubMed
-
- Nguyen NT, Thosani NC, Canto MI, Chang K, Lipham J, Abu Dayyeh B et al (2022) The American Foregut Society white paper on the endoscopic classification of esophagogastric junction integrity. Foregut J Am Foregut Soc 2(4):339–348. 10.1177/26345161221126961
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
