

Randomized Trials of Renal Denervation for Uncontrolled Hypertension: An Updated Meta-Analysis
- PMID: 39140334
- PMCID: PMC11963938
- DOI: 10.1161/JAHA.124.034910
Randomized Trials of Renal Denervation for Uncontrolled Hypertension: An Updated Meta-Analysis
Abstract
Background: Despite optimal medical therapy, a significant proportion of patients' blood pressure remains uncontrolled. Catheter-based renal denervation (RDN) has been proposed as a potential intervention for uncontrolled hypertension. We conducted an updated meta-analysis to assess the efficacy and safety of RDN in patients with uncontrolled hypertension, with emphasis on the differential effect of RDN in patients on and off antihypertensive medications.
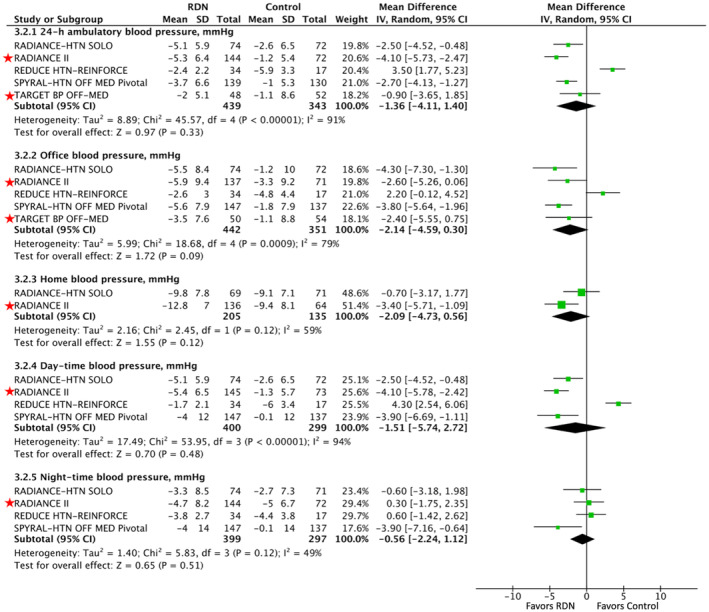
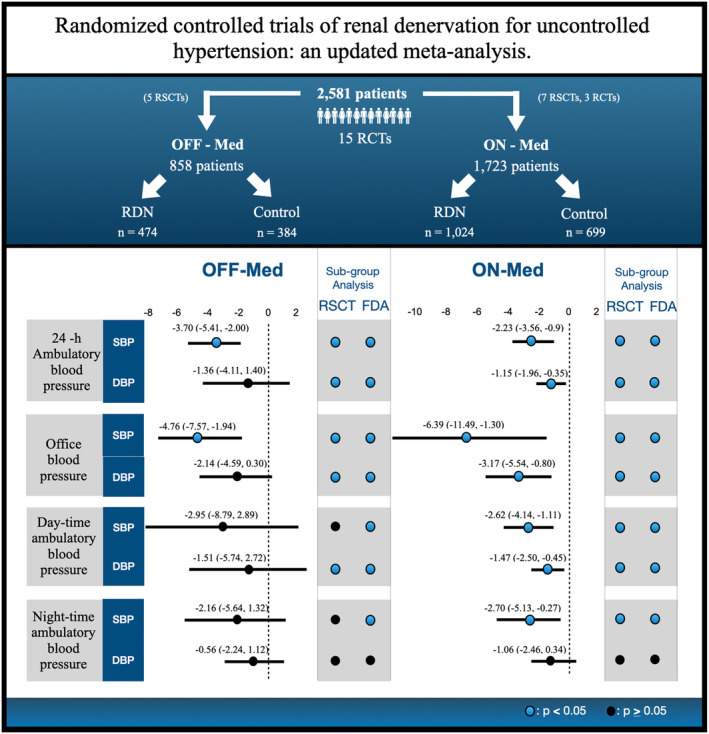
Methods and results: Online databases were searched to identify randomized clinical trials comparing efficacy and safety of RDN versus control in patients with uncontrolled hypertension. Subgroup analyses were conducted for sham-controlled trials and studies that used RDN devices that have gained or are currently seeking US Food and Drug Administration approval. Fifteen trials with 2581 patients (RDN, 1723; sham, 858) were included. In patients off antihypertensive medications undergoing RDN, a significant reduction in 24-hour ambulatory (-3.70 [95% CI, -5.41 to -2.00] mm Hg), office (-4.76 [95% CI, -7.57 to -1.94] mm Hg), and home (-3.28 [95% CI, -5.96 to -0.61] mm Hg) systolic blood pressures was noted. In patients on antihypertensive medications, a significant reduction was observed in 24-hour ambulatory (-2.23 [95% CI, -3.56 to -0.90] mm Hg), office (-6.39 [95% CI, -11.49 to -1.30]), home (-6.08 [95% CI, -11.54 to -0.61] mm Hg), daytime (-2.62 [95% CI, -4.14 to -1.11]), and nighttime (-2.70 [95% CI, -5.13 to -0.27]) systolic blood pressures, as well as 24-hour ambulatory (-1.16 [95% CI, -1.96 to -0.35]), office (-3.17 [95% CI, -5.54 to -0.80]), and daytime (-1.47 [95% CI, -2.50 to -0.27]) diastolic blood pressures.
Conclusions: RDN significantly lowers blood pressure in patients with uncontrolled hypertension, in patients off and on antihypertensive medications, with a favorable safety profile. The efficacy of RDN was consistent in sham-controlled trials and contemporary trials using US Food and Drug Administration-approved devices.
Keywords: denervation; hypertension; renal; renal denervation; uncontrolled.
Figures






Comment in
-
Catheter-Based Renal Denervation Ready for the Management of Hypertension: Evidence, Challenges, and Perspectives.J Am Heart Assoc. 2024 Aug 20;13(16):e037099. doi: 10.1161/JAHA.124.037099. Epub 2024 Aug 14. J Am Heart Assoc. 2024. PMID: 39140342 Free PMC article. No abstract available.
References
-
- Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, Toto RD, White A, Cushman WC, White W, Sica D, et al. Resistant hypertension: diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Hypertension. 2008;51:1403–1419. doi: 10.1161/HYPERTENSIONAHA.108.189141 - DOI - PubMed
-
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, Clement DL, Coca A, de Simone G, Dominiczak A, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur Heart J. 2018;39:3021–3104. doi: 10.1093/eurheartj/ehy339 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
