

Identifying the primary tumour in patients with cancer of unknown primary (CUP) using [18F]FDG PET/CT: a systematic review and individual patient data meta-analysis
- PMID: 39141069
- PMCID: PMC11599304
- DOI: 10.1007/s00259-024-06860-1
Identifying the primary tumour in patients with cancer of unknown primary (CUP) using [18F]FDG PET/CT: a systematic review and individual patient data meta-analysis
Abstract
Purpose: In this systematic review and individual patient data (IPD) meta-analysis, we analysed the diagnostic performance of [18F]FDG PET/CT in detecting primary tumours in patients with CUP and evaluated whether the location of the predominant metastatic site influences the diagnostic performance.
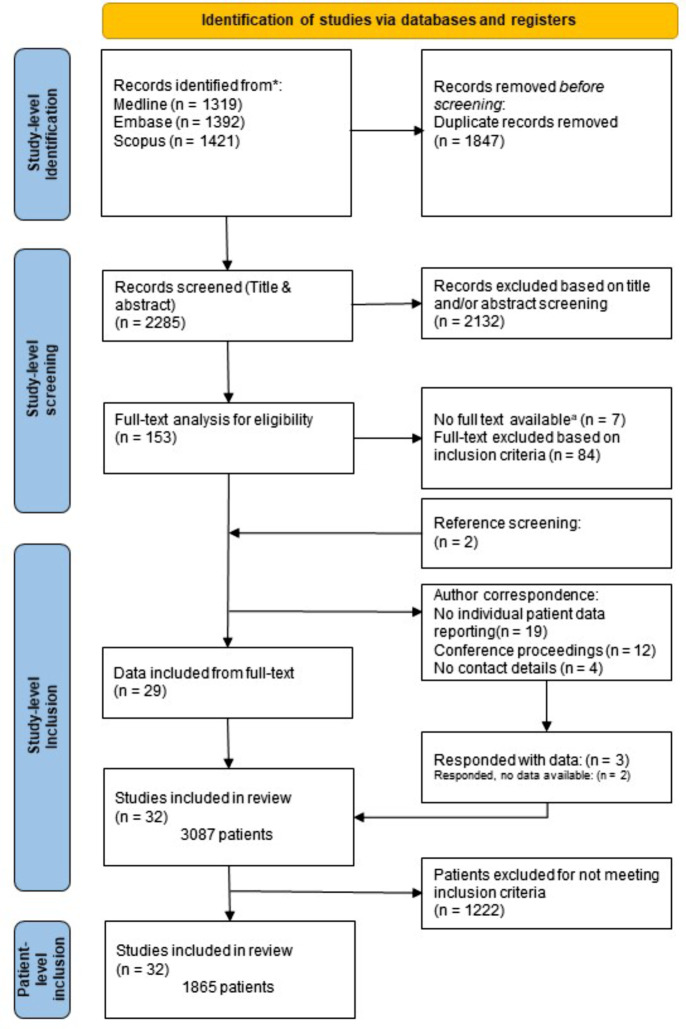
Methods: A systematic literature search from January 2005 to February 2024 was performed to identify articles describing the diagnostic performance of [18F]FDG PET/CT for primary tumour detection in CUP. Individual patient data retrieved from original articles or obtained from corresponding authors were grouped by the predominant metastatic site. The diagnostic performance of [18F]FDG PET/CT in detecting the underlying primary tumour was compared between predominant metastatic sites.
Results: A total of 1865 patients from 32 studies were included. The largest subgroup included patients with predominant bone metastases (n = 622), followed by liver (n = 369), lymph node (n = 358), brain (n = 316), peritoneal (n = 70), lung (n = 67), and soft tissue (n = 23) metastases, leaving a small group of other/undefined metastases (n = 40). [18F]FDG PET/CT resulted in pooled detection rates to identify the primary tumour of 0.74 (for patients with predominant brain metastases), 0.54 (liver-predominant), 0.49 (bone-predominant), 0.46 (lung-predominant), 0.38 (peritoneal-predominant), 0.37 (lymph node-predominant), and 0.35 (soft-tissue-predominant).
Conclusion: This individual patient data meta-analysis suggests that the ability of [18F]FDG PET/CT to identify the primary tumour in CUP depends on the distribution of metastatic sites. This finding emphasises the need for more tailored diagnostic approaches in different patient populations. In addition, alternative diagnostic tools, such as new PET tracers or whole-body (PET/)MRI, should be investigated.
Keywords: Cancer of unknown primary; Meta-analysis; Molecular imaging; Oncology; [18F]FDG PET/CT.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This is a systematic review and individual patient data meta-analysis, for which ethical approval is not required. Consent to participate: Not applicable. Consent to publish: Not applicable. Competing interests: The authors have no relevant financial or non-financial interests to disclose.
Figures



References
-
- Varadhachary GR, Raber MN. Cancer of unknown primary site. N Engl J Med. 2014;371:757–65. 10.1056/nejmra1303917. - PubMed
-
- Schroten-Loef C, Verhoeven RHA, de Hingh I, van de Wouw AJ, van Laarhoven HWM, Lemmens V. Unknown primary carcinoma in the Netherlands: decrease in incidence and survival times remain poor between 2000 and 2012. Eur J Cancer. 2018;101:77–86. 10.1016/j.ejca.2018.06.032. - PubMed
-
- Hemminki K, Bevier M, Hemminki A, Sundquist J. Survival in cancer of unknown primary site: population-based analysis by site and histology. Ann Oncol. 2012;23:1854–63. 10.1093/annonc/mdr536. - PubMed
-
- Pavlidis N, Pentheroudakis G. Cancer of unknown primary site. Lancet. 2012;379:1428–35. 10.1016/s0140-6736(11)61178-1. - PubMed
-
- Pentheroudakis G, Greco FA, Pavlidis N. Molecular assignment of tissue of origin in cancer of unknown primary may not predict response to therapy or outcome: a systematic literature review. Cancer Treat Rev. 2009;35:221–7. 10.1016/j.ctrv.2008.10.003. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
