

Targeting NGF but not VEGFR1 or BDNF signaling reduces endometriosis-associated pain in mice
- PMID: 39142441
- PMCID: PMC12225929
- DOI: 10.1016/j.jare.2024.08.017
Targeting NGF but not VEGFR1 or BDNF signaling reduces endometriosis-associated pain in mice
Abstract
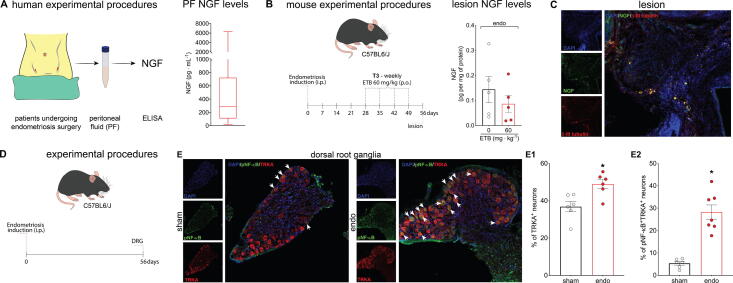
Introduction: Endometriosis is a chronic inflammatory disease that affects ∼10 % of women. A significant fraction of patients experience limited or no efficacy with current therapies. Tissue adjacent to endometriosis lesions often exhibits increased neurite and vascular density, suggesting that disease pathology involves neurotrophic activity and angiogenesis.
Objectives: We aim to evaluate the potential for key tyrosine-kinase-receptor-coupled neurotrophic molecules to contribute to endometriosis-associated pain in mice.
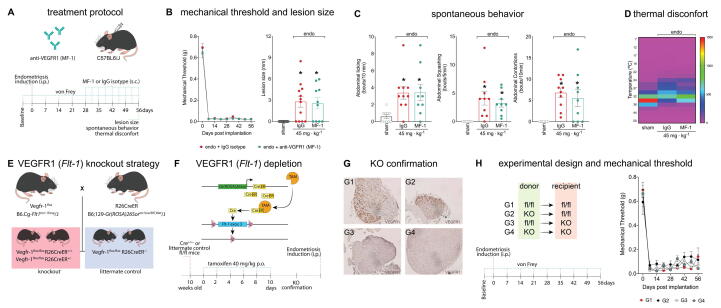
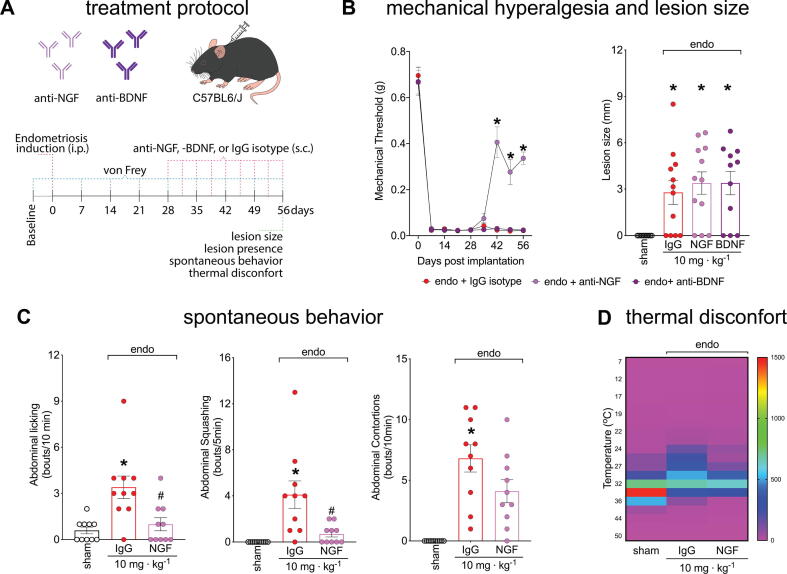
Methods: Peritoneal fluid was collected from endometriosis patients undergoing surgery and the levels of NGF and VEGFR1 regulators (VEGFA, VEGFB, PLGF, and sVEGFR1) were quantified by ELISA. VEGFR1 regulator concentrations were used to calculate VEGFR1 occupancy. We used genetic depletion, neutralizing antibodies, and pharmacological approaches to specifically block neurotrophic ligands (NGF or BDNF) or receptors (VEGFR1, TRKs) in a murine model of endometriosis-associated pain. Endometriosis-associated pain was measured using von Frey filaments, quantification of spontaneous abdominal pain-related behavior, and thermal discomfort. Disease parameters were evaluated by lesion size and prevalence. To evaluate potential toxicity, we measured the effect of entrectinib dose and schedule on body weight, liver and kidney function, and bone structure (via micro-CT).
Results: We found that entrectinib (pan-Trk inhibitor) or anti-NGF treatments reduced evoked pain, spontaneous pain, and thermal discomfort. In contrast, even though calculated receptor occupancy revealed that VEGFR1 agonist levels are sufficient to support signaling, blocking VEGFR1 via antibody or tamoxifen-induced knockout did not reduce pain or lesion size in mice. Targeting BDNF-TrkB with an anti-BDNF antibody also proved ineffective. Notably, changing dosing schedule to once weekly eliminated entrectinib-induced bone-loss without decreasing efficacy against pain.
Conclusions: This suggests NGF-TrkA signaling, but not BDNF-TrkB or VEGF-VEGFR1, mediates endometriosis-associated pain. Moreover, entrectinib blocks endometriosis-associated pain and reduces lesion sizes. Our results also indicated that entrectinib-like molecules are promising candidates for endometriosis treatment.
Keywords: BDNF; Neurotrophins; VEGF; VEGFR1; Visceral pain.
Copyright © 2024. Published by Elsevier B.V.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
