

Oxygen-Enhanced MRI Detects Incidence, Onset, and Heterogeneity of Radiation-Induced Hypoxia Modification in HPV-Associated Oropharyngeal Cancer
- PMID: 39142654
- PMCID: PMC11654720
- DOI: 10.1158/1078-0432.CCR-24-1170
Oxygen-Enhanced MRI Detects Incidence, Onset, and Heterogeneity of Radiation-Induced Hypoxia Modification in HPV-Associated Oropharyngeal Cancer
Abstract
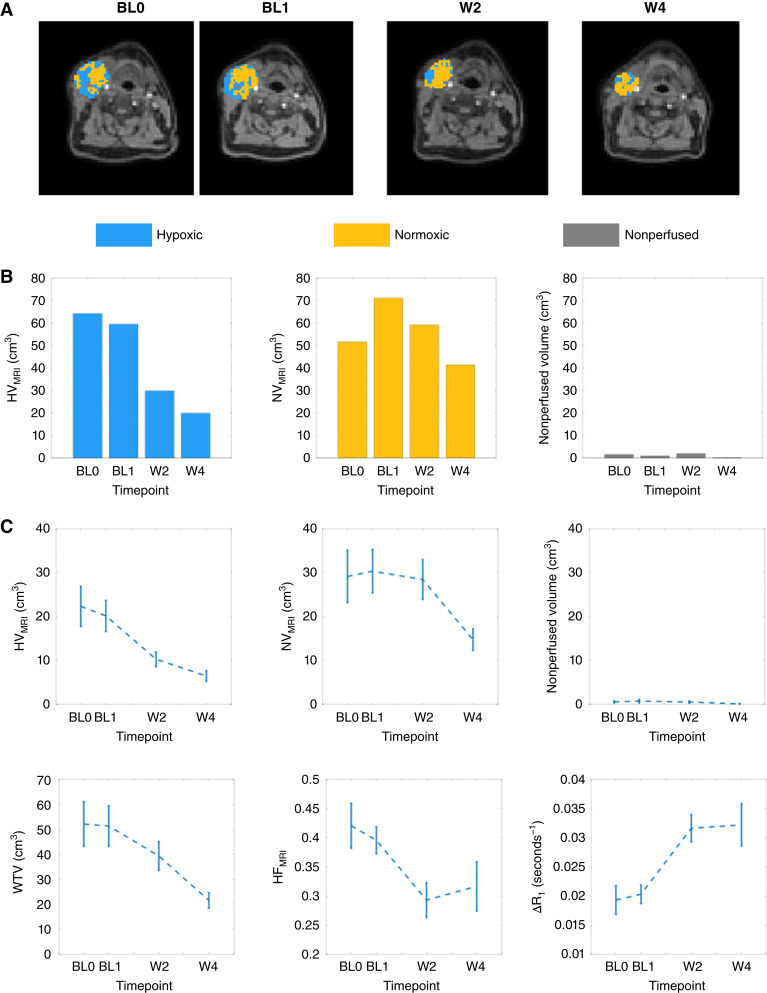
Purpose: Hypoxia mediates treatment resistance in solid tumors. We evaluated if oxygen-enhanced MRI-derived hypoxic volume (HVMRI) is repeatable and can detect radiotherapy-induced hypoxia modification in human papillomavirus-associated oropharyngeal head and neck squamous cell cancer.
Experimental design: A total of 27 patients were recruited prospectively between March 2021 and January 2024. HVMRI was measured in primary and nodal tumors prior to standard-of-care (chemo)radiotherapy and then at weeks 2 and 4 (W2 and W4) into therapy. Two pretreatment scans assessed biomarker within-subject coefficient of variation and repeatability coefficient (RC). Cohort treatment response was measured using mixed-effects modeling. Responding lesions were identified by comparing HVMRI change with RC limits of agreement.
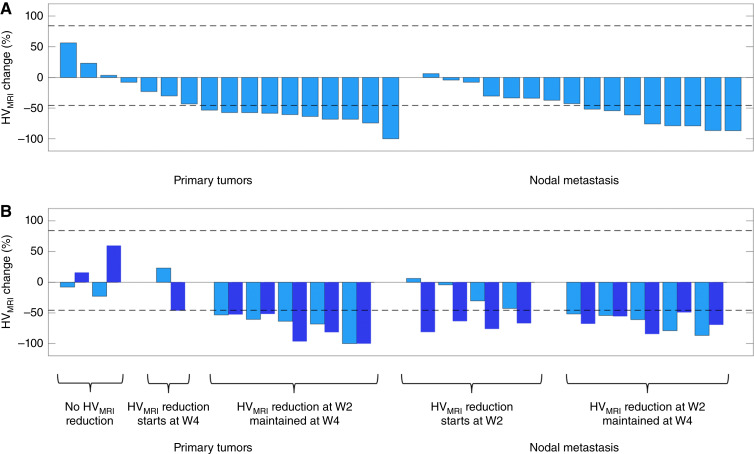
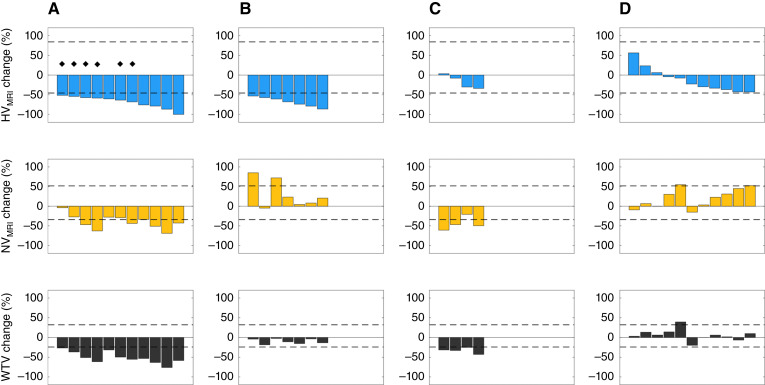
Results: Oxygen-enhanced MRI identified hypoxia in all lesions. The HVMRI within-subject coefficient of variation was 24.6%, and RC limits of agreement were -45.7% to 84.1%. A cohort median pretreatment HVMRI of 11.3 cm3 reduced to 6.9 cm3 at W2 and 5.9 cm3 at W4 (both P < 0.001). HVMRI was reduced in 54.5% of individual lesions by W2 and in 88.2% by W4. All lesions with W2 hypoxia reduction showed persistent modification at W4. HVMRI reduced in some lesions that showed no overall volume change. Hypoxia modification was discordant between primary and nodal tumors in 50.0% of patients.
Conclusions: Radiation-induced hypoxia modification can occur as early as W2, but onset varies between patients and was not necessarily associated with overall size change. Half of all patients had discordant changes in primary and nodal tumors. These findings have implications for patient selection and timing of dose de-escalation strategies in human papillomavirus-associated oropharyngeal carcinoma. See related commentary by Mason, p. 5503.
©2024 American Association for Cancer Research.
Conflict of interest statement
M.J. Dubec reports grants from Medical Research Council and Cancer Research UK during the conduct of the study. A. Choudhury reports grants from UK Research Innovation and Cancer Research UK during the conduct of the study as well as grants from Prostate Cancer UK, The Urology Foundation, Action Bladder Cancer, and Elekta AB and personal fees from BMJ, Merck, AstraZeneca, and Bayer outside the submitted work. J.C. Matthews reports grants from UK Medical Research Council during the conduct of the study. G.J.M. Parker reports personal fees and other support from Bioxydyn Limited, other support from Quantitative Imaging Limited and Queen Square Analytics Limited, and grants from GSK outside the submitted work. A. McPartlin reports personal fees from Philips Healthcare outside the submitted work. J.P.B. O’Connor reports grants from Cancer Research UK during the conduct of the study. No conflicts of interest were disclosed by the other authors.
Figures
References
-
- Harris AL. Hypoxia—a key regulatory factor in tumour growth. Nat Rev Cancer 2002;2:38–47. - PubMed
-
- Overgaard J. Hypoxic radiosensitization: adored and ignored. J Clin Oncol 2007;25:4066–74. - PubMed
-
- Minassian LM, Cotechini T, Huitema E, Graham CH. Hypoxia-induced resistance to chemotherapy in cancer. Adv Exp Med Biol 2019;1136:123–39. - PubMed
-
- Horsman MR, Mortensen LS, Petersen JB, Busk M, Overgaard J. Imaging hypoxia to improve radiotherapy outcome. Nat Rev Clin Oncol 2012;9:674–87. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
