

Comprehensive genetic profiling and molecularly guided treatment for patients with primary CNS tumors
- PMID: 39143272
- PMCID: PMC11324882
- DOI: 10.1038/s41698-024-00674-y
Comprehensive genetic profiling and molecularly guided treatment for patients with primary CNS tumors
Abstract
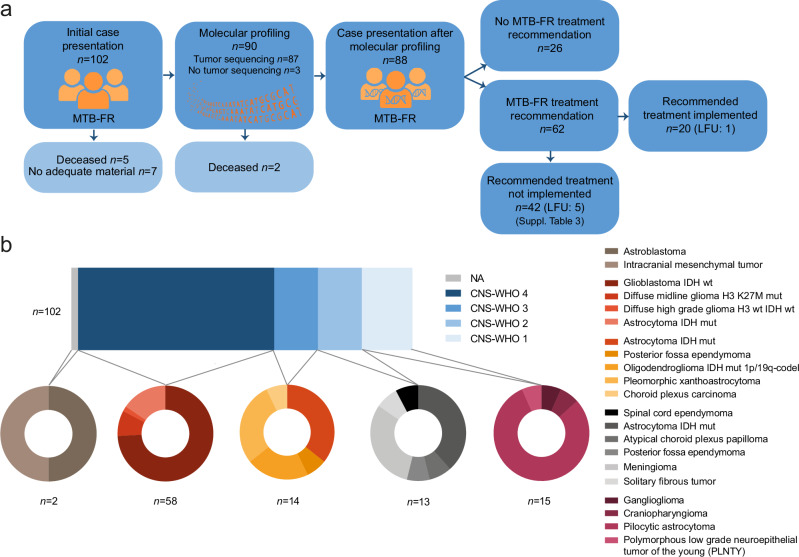
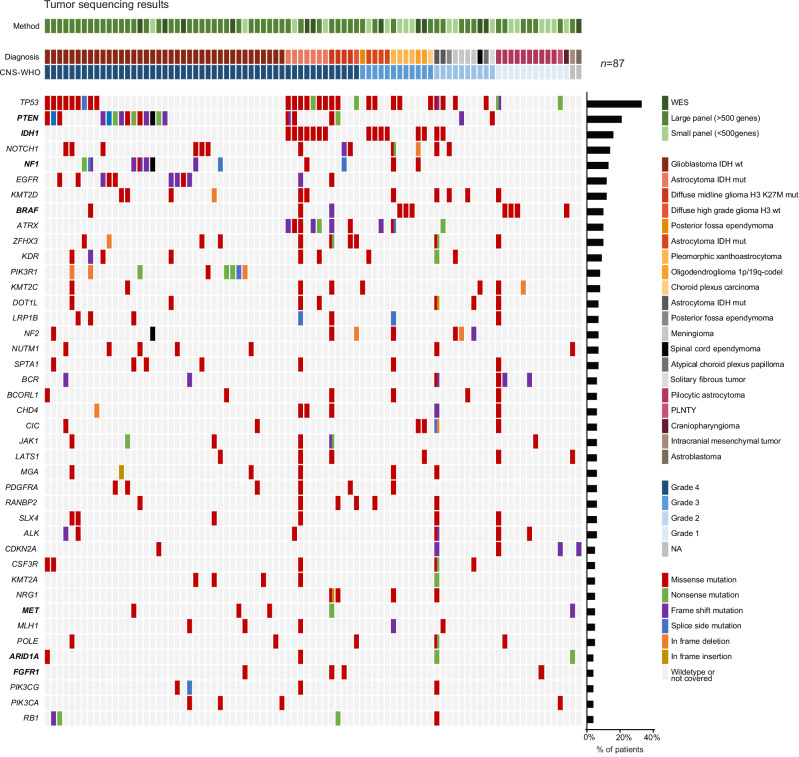
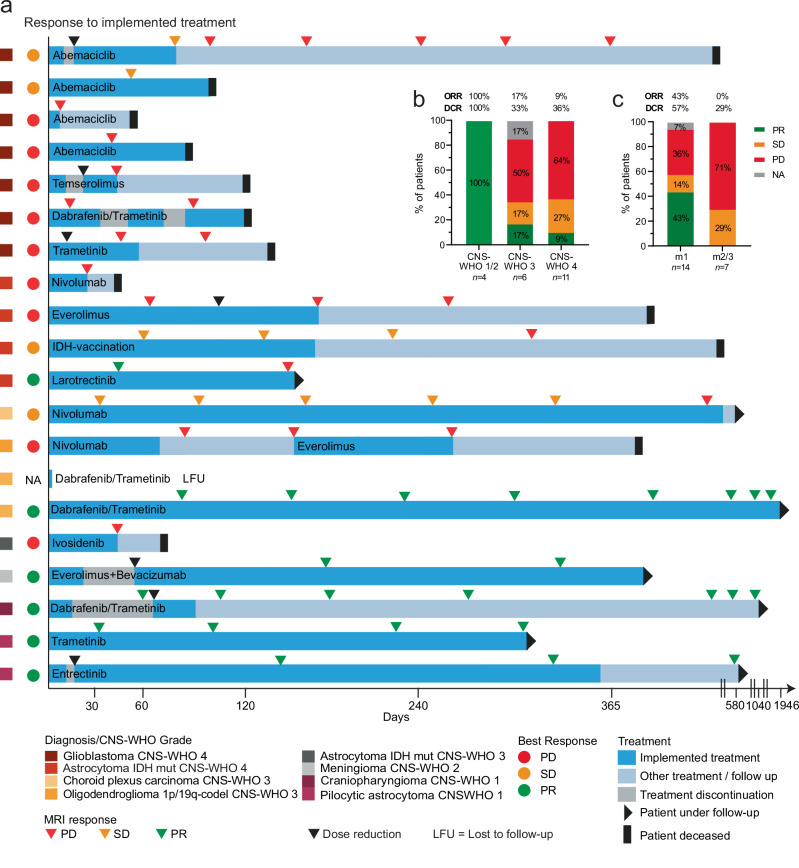
Despite major advances in molecular profiling and classification of primary brain tumors, personalized treatment remains limited for most patients. Here, we explored the feasibility of individual molecular profiling and the efficacy of biomarker-guided therapy for adult patients with primary brain cancers in the real-world setting within the molecular tumor board Freiburg, Germany. We analyzed genetic profiles, personalized treatment recommendations, and clinical outcomes of 102 patients with 21 brain tumor types. Alterations in the cell cycle, BRAF, and mTOR pathways most frequently led to personalized treatment recommendations. Molecularly informed therapies were recommended in 71% and implemented in 32% of patients with completed molecular diagnostics. The disease control rate following targeted treatment was 50% and the overall response rate was 30%, with a progression-free survival 2/1 ratio of at least 1.3 in 31% of patients. This study highlights the efficacy of molecularly guided treatment and the need for biomarker-stratified trials in brain cancers.
© 2024. The Author(s).
Conflict of interest statement
J.C.K. does not report any conflicts of interest. F.S. receives research funding from Gilead Sciences, Roche Sequencing Solutions, and Takeda, and received Honoraria from AstraZeneca and Servier. Any other authors do not report any conflicts of interest.
Figures

References
-
- Le Tourneau, C. et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): a multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol.16, 1324–1334 (2015). 10.1016/S1470-2045(15)00188-6 - DOI - PubMed
-
- Massard, C. et al. High-throughput genomics and clinical outcome in hard-to-treat advanced cancers: results of the MOSCATO 01 Trial. Cancer Discov.7, 586–595 (2017). 10.1158/2159-8290.CD-16-1396 - DOI - PubMed
Grants and funding
- SCHE 1807/3-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- 441891347/Deutsche Forschungsgemeinschaft (German Research Foundation)
- CRC1479/Deutsche Forschungsgemeinschaft (German Research Foundation)
- 2018_A38/Else Kröner-Fresenius-Stiftung (Else Kroner-Fresenius Foundation)
- 01EO2103/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
