

Proteomics identifies potential immunological drivers of postinfection brain atrophy and cognitive decline
- PMID: 39143319
- PMCID: PMC11408246
- DOI: 10.1038/s43587-024-00682-4
Proteomics identifies potential immunological drivers of postinfection brain atrophy and cognitive decline
Abstract
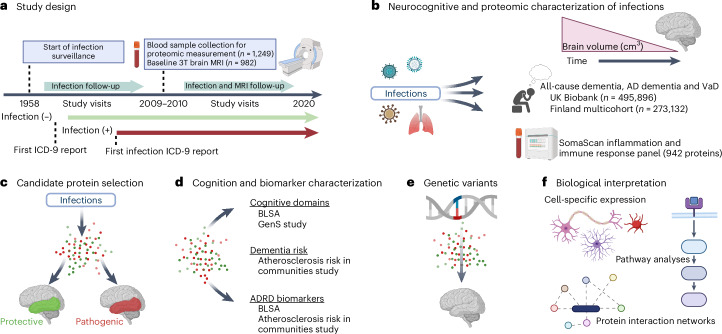
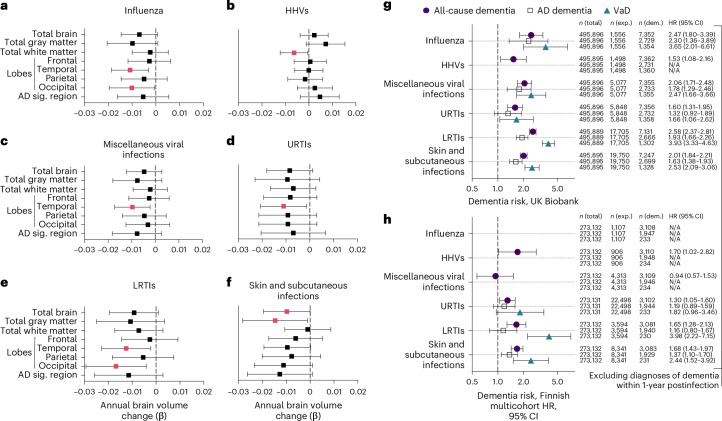
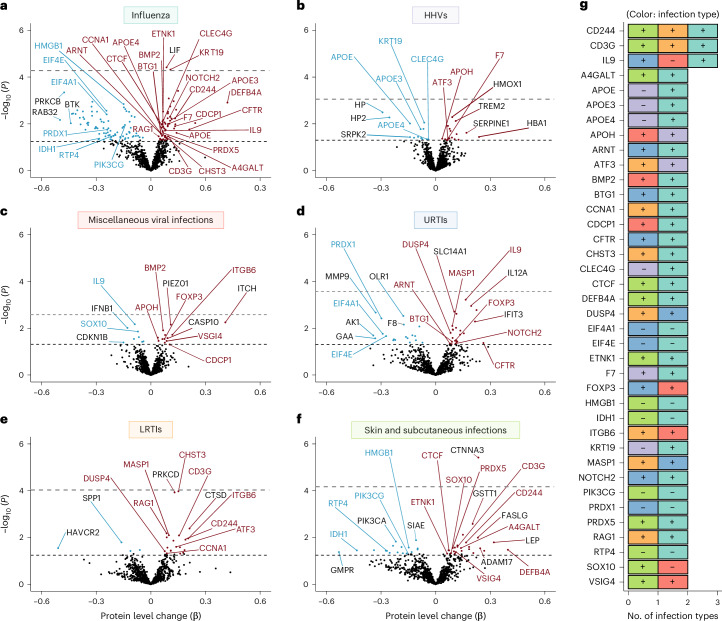
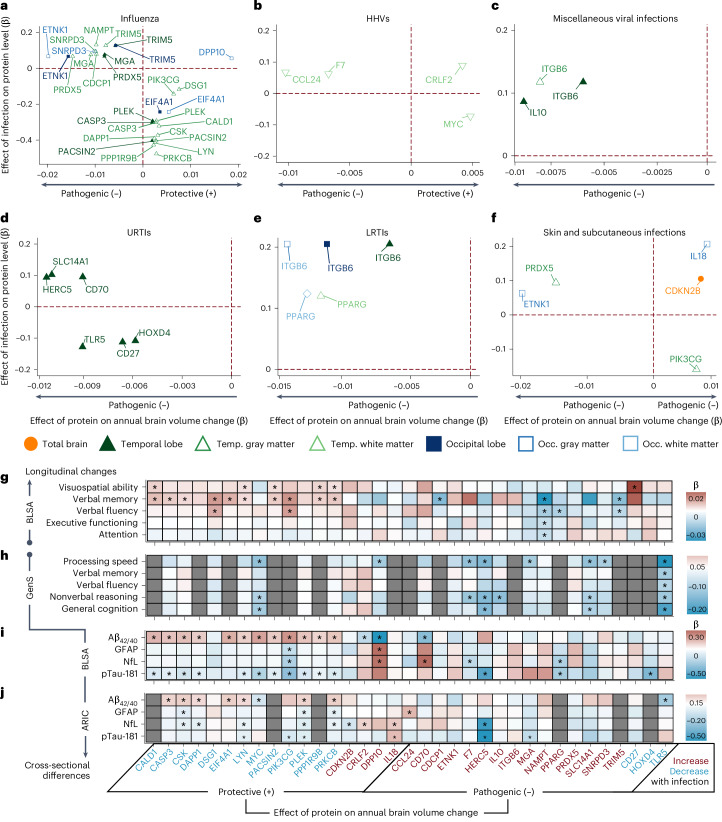
Infections have been associated with the incidence of Alzheimer disease and related dementias, but the mechanisms responsible for these associations remain unclear. Using a multicohort approach, we found that influenza, viral, respiratory, and skin and subcutaneous infections were associated with increased long-term dementia risk. These infections were also associated with region-specific brain volume loss, most commonly in the temporal lobe. We identified 260 out of 942 immunologically relevant proteins in plasma that were differentially expressed in individuals with an infection history. Of the infection-related proteins, 35 predicted volumetric changes in brain regions vulnerable to infection-specific atrophy. Several of these proteins, including PIK3CG, PACSIN2, and PRKCB, were related to cognitive decline and plasma biomarkers of dementia (Aβ42/40, GFAP, NfL, pTau-181). Genetic variants that influenced expression of immunologically relevant infection-related proteins, including ITGB6 and TLR5, predicted brain volume loss. Our findings support the role of infections in dementia risk and identify molecular mediators by which infections may contribute to neurodegeneration.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
M.A.N. and C.X.A.’s participation in this project was part of a competitive contract awarded to DataTecnica LLC by the NIH to support open science research. M.A.N. also currently serves on the scientific advisory board for Character Bio Inc. and Neuron23 Inc. The remaining authors declare no competing interests.
Figures










References
MeSH terms
Substances
Grants and funding
- Z01 AG000949/ImNIH/Intramural NIH HHS/United States
- 75N92022D00002/HL/NHLBI NIH HHS/United States
- U01 HL096917/HL/NHLBI NIH HHS/United States
- 1ZIAAG000348/U.S. Department of Health & Human Services | NIH | National Institute on Aging (U.S. National Institute on Aging)
- R01AG056477/U.S. Department of Health & Human Services | NIH | National Institute on Aging (U.S. National Institute on Aging)
- 75N92022D00004/HL/NHLBI NIH HHS/United States
- 1ZIAAG000349/U.S. Department of Health & Human Services | NIH | National Institute on Aging (U.S. National Institute on Aging)
- U01 HL096814/HL/NHLBI NIH HHS/United States
- ZIA AG000348/ImNIH/Intramural NIH HHS/United States
- 75N92022D00003/HL/NHLBI NIH HHS/United States
- 75N92022D00005/HL/NHLBI NIH HHS/United States
- 75N95020D00014/DA/NIDA NIH HHS/United States
- 75N92022D00001/HL/NHLBI NIH HHS/United States
- R01 AG056477/AG/NIA NIH HHS/United States
- ZIA AG000349/ImNIH/Intramural NIH HHS/United States
- U01 HL096812/HL/NHLBI NIH HHS/United States
- 1ZIAAG00935/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
- R00 AG070109/AG/NIA NIH HHS/United States
- U01 HL096902/HL/NHLBI NIH HHS/United States
- Z01-AG000949-02/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
- 1ZIANS003154/U.S. Department of Health & Human Services | NIH | National Institute of Neurological Disorders and Stroke (NINDS)
- ZIA AG000935/ImNIH/Intramural NIH HHS/United States
- R01 AG059716/AG/NIA NIH HHS/United States
- RF1 AG054409/AG/NIA NIH HHS/United States
- ZIA NS003154/ImNIH/Intramural NIH HHS/United States
- WT_/Wellcome Trust/United Kingdom
- U01 HL096899/HL/NHLBI NIH HHS/United States
- R00 AG052830/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
