

Optimal methods of vitamin D supplementation to prevent acute respiratory infections: a systematic review, dose-response and pairwise meta-analysis of randomized controlled trials
- PMID: 39143549
- PMCID: PMC11323636
- DOI: 10.1186/s12937-024-00990-w
Optimal methods of vitamin D supplementation to prevent acute respiratory infections: a systematic review, dose-response and pairwise meta-analysis of randomized controlled trials
Abstract
Background: Vitamin D supplementation may prevent acute respiratory infections (ARIs). This study aimed to identify the optimal methods of vitamin D supplementation.
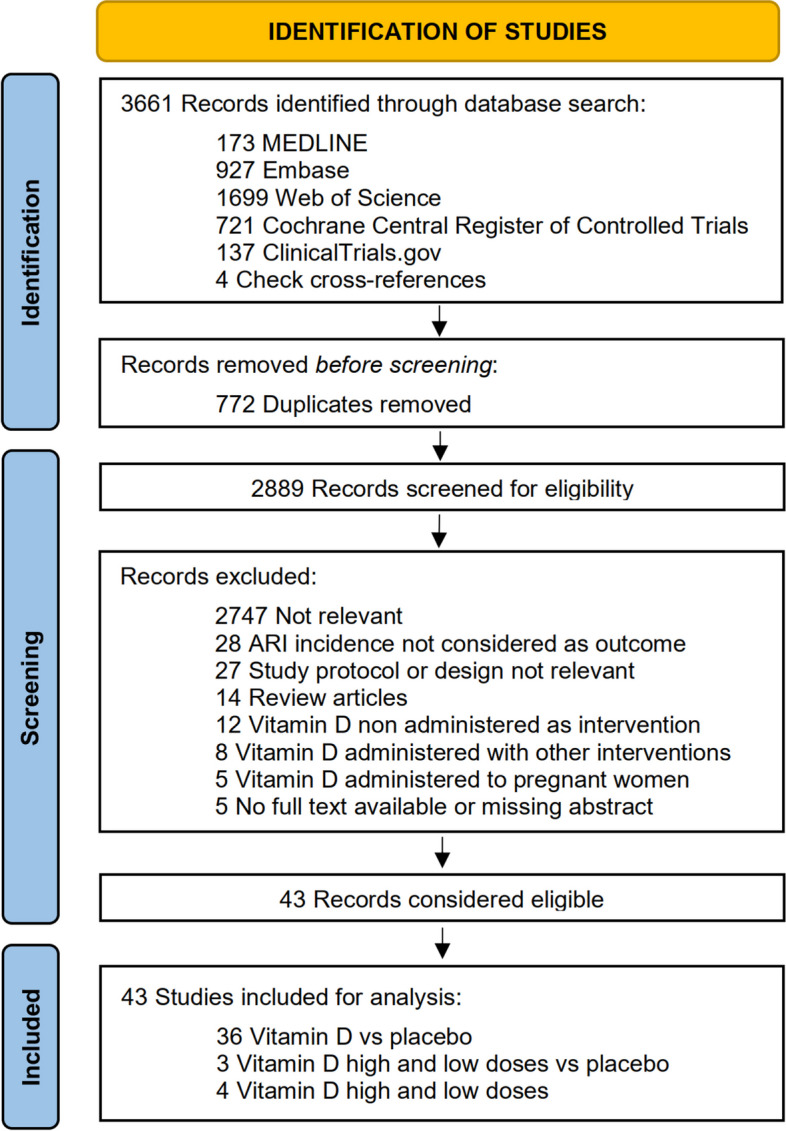
Methods: PubMed, Embase, Cochrane Central Register of Controlled Trials, Web of Science, and the ClinicalTrials.gov registry were searched from database inception through July 13, 2023. Randomized-controlled trials (RCTs) were included. Data were pooled using random-effects model. The primary outcome was the proportion of participants with one or more ARIs.
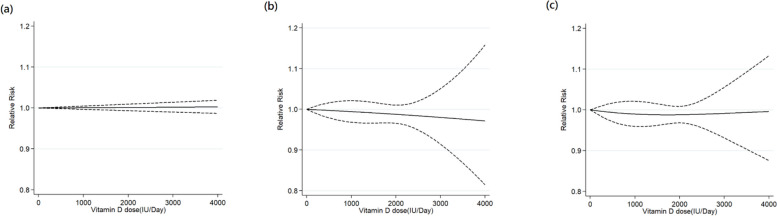
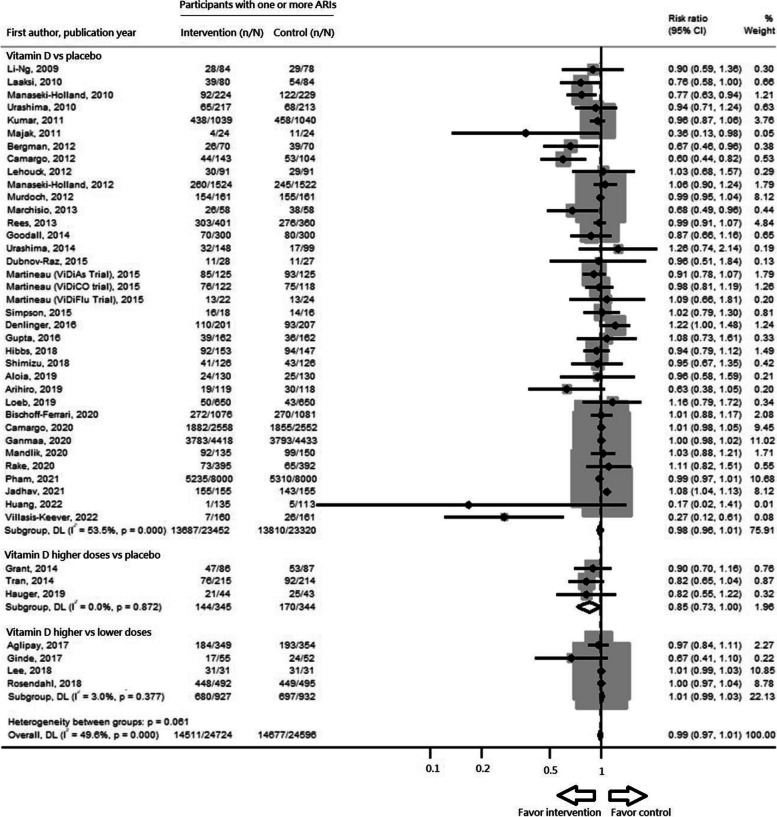
Results: The analysis included 43 RCTs with 49320 participants. Forty RCTs were considered to be at low risk for bias. The main pairwise meta-analysis indicated there were no significant preventive effects of vitamin D supplementation against ARIs (risk ratio [RR]: 0.99, 95% confidence interval [CI]: 0.97 to 1.01, I2 = 49.6%). The subgroup dose-response meta-analysis indicated that the optimal vitamin D supplementation doses ranged between 400-1200 IU/day for both summer-sparing and winter-dominant subgroups. The subgroup pairwise meta-analysis also revealed significant preventive effects of vitamin D supplementation in subgroups of daily dosing (RR: 0.92, 95% CI: 0.85 to 0.99, I2 = 55.7%, number needed to treat [NNT]: 36), trials duration < 4 months (RR: 0.81, 95% CI: 0.67 to 0.97, I2 = 48.8%, NNT: 16), summer-sparing seasons (RR: 0.85, 95% CI: 0.74 to 0.98, I2 = 55.8%, NNT: 26), and winter-dominant seasons (RR: 0.79, 95% CI: 0.71 to 0.89, I2 = 9.7%, NNT: 10).
Conclusion: Vitamin D supplementation may slightly prevent ARIs when taken daily at doses between 400 and 1200 IU/d during spring, autumn, or winter, which should be further examined in future clinical trials.
Keywords: Acute respiratory infection; Dosage; Dose–response analysis; Meta-analysis; Seasonal effects; Vitamin D.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Global Health Estimates: Life expectancy and leading causes of death and disability. https://www.who.int/data/gho/data/themes/mortality-and-global-health-est.... Accessed on 13 May 2024.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
