

The clinical impacts of lung microbiome in bronchiectasis with fixed airflow obstruction: a prospective cohort study
- PMID: 39143556
- PMCID: PMC11325704
- DOI: 10.1186/s12931-024-02931-x
The clinical impacts of lung microbiome in bronchiectasis with fixed airflow obstruction: a prospective cohort study
Abstract
Background: Airflow obstruction is a hallmark of disease severity and prognosis in bronchiectasis. The relationship between lung microbiota, airway inflammation, and outcomes in bronchiectasis with fixed airflow obstruction (FAO) remains unclear. This study explores these interactions in bronchiectasis patients, with and without FAO, and compares them to those diagnosed with chronic obstructive pulmonary disease (COPD).
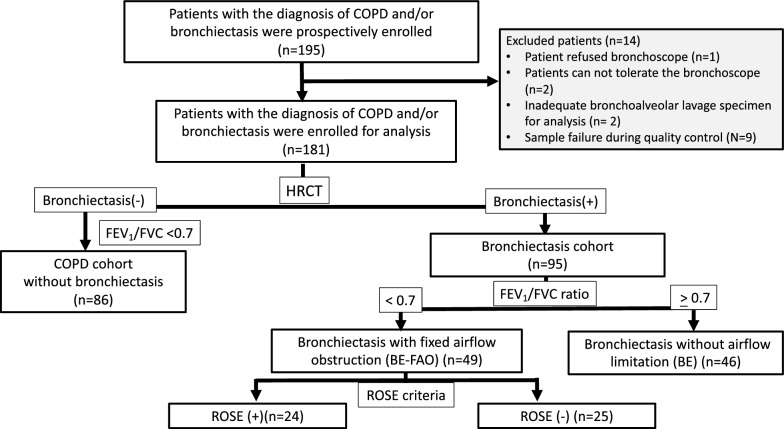
Methods: This prospective observational study in Taiwan enrolled patients with either bronchiectasis or COPD. To analyze the lung microbiome and assess inflammatory markers, bronchoalveolar lavage (BAL) samples were collected for 16S rRNA gene sequencing. The study cohort comprised 181 patients: 86 with COPD, 46 with bronchiectasis, and 49 with bronchiectasis and FAO, as confirmed by spirometry.
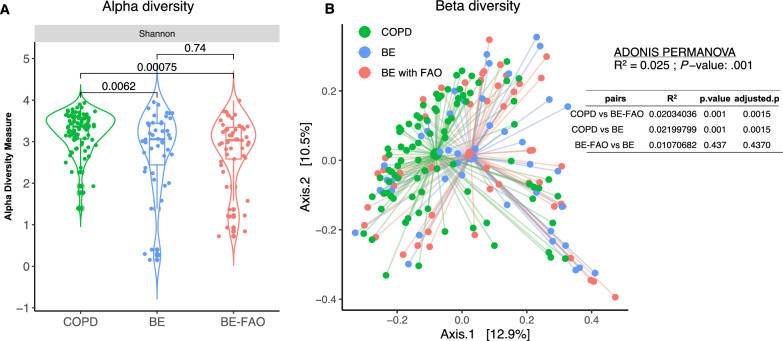
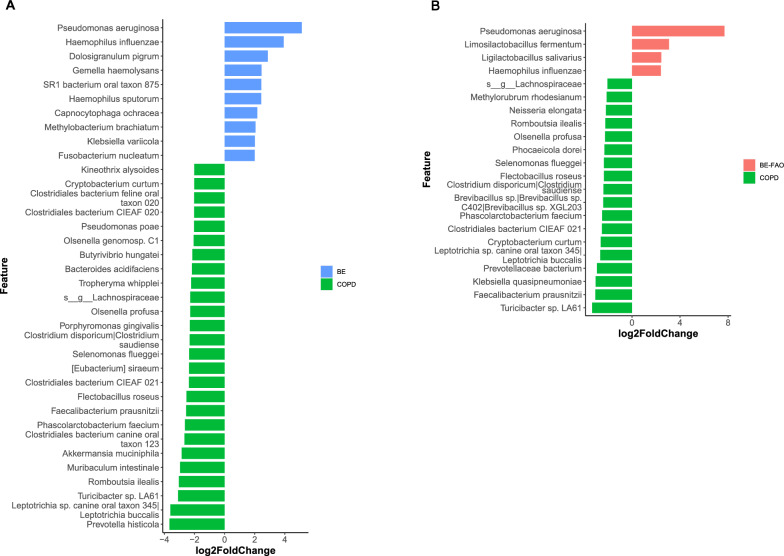
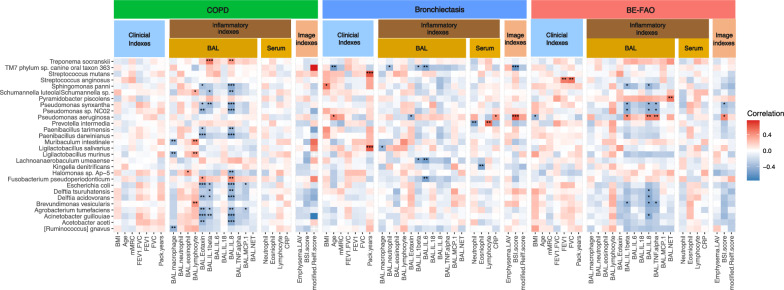
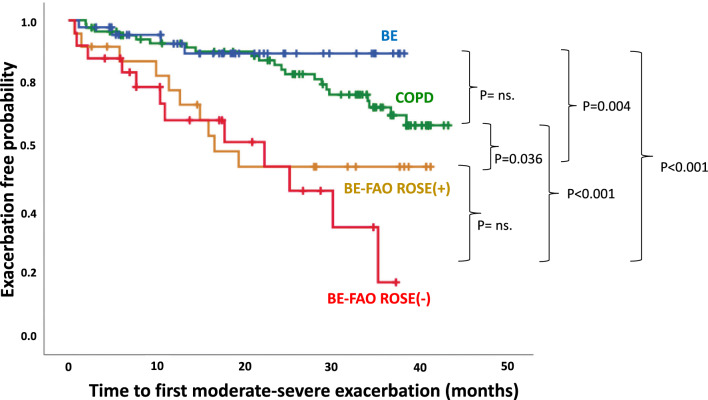
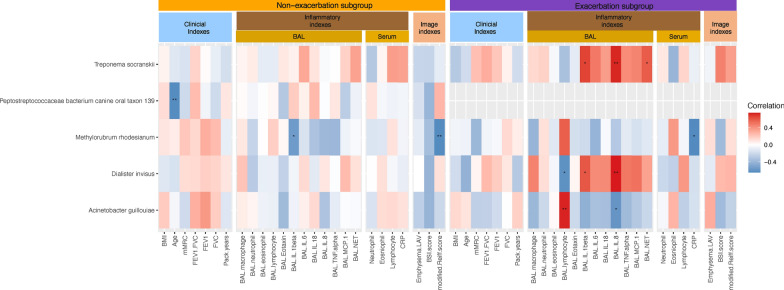
Results: Patients with bronchiectasis, with or without FAO, had similar microbiome profiles characterized by reduced alpha diversity and a predominance of Proteobacteria, distinctly different from COPD patients who exhibited more Firmicutes, greater diversity, and more commensal taxa. Furthermore, compared to COPD and bronchiectasis without FAO, bronchiectasis with FAO showed more severe disease and a higher risk of exacerbations. A significant correlation was found between the presence of Pseudomonas aeruginosa and increased airway neutrophilic inflammation such as Interleukin [IL]-1β, IL-8, and tumor necrosis factor-alpha [TNF]-α, as well as with higher bronchiectasis severity, which might contribute to an increased risk of exacerbations. Moreover, in bronchiectasis patients with FAO, the ROSE (Radiology, Obstruction, Symptoms, and Exposure) criteria were employed to classify individuals as either ROSE (+) or ROSE (-), based on smoking history. This classification highlighted differences in clinical features, inflammatory profiles, and slight microbiome variations between ROSE (-) and ROSE (+) patients, suggesting diverse endotypes within the bronchiectasis with FAO group.
Conclusion: Bronchiectasis patients with FAO may exhibit two distinct endotypes, as defined by ROSE criteria, characterized by greater disease severity and a lung microbiome more similar to bronchiectasis without FAO than to COPD. The significant correlation between Pseudomonas aeruginosa colonization and increased airway neutrophilic inflammation, as well as disease severity, underscores the clinical relevance of microbial patterns. This finding reinforces the potential role of these patterns in the progression and exacerbations of bronchiectasis with FAO.
Keywords: Bronchiectasis; Bronchoalveolar lavage; COPD; Fixed airflow obstruction; Lung microbiota; Neutrophilic inflammation; ROSE criteria.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
