

Prehospital treatment of severely burned patients: a retrospective analysis of patients admitted to the Berlin burn centre
- PMID: 39143646
- PMCID: PMC11323598
- DOI: 10.1186/s13049-024-01239-5
Prehospital treatment of severely burned patients: a retrospective analysis of patients admitted to the Berlin burn centre
Abstract
Background: Prehospital management of severely burned patients is extremely challenging. It should include adequate analgesia, decision-making on the necessity of prehospital endotracheal intubation and the administration of crystalloid fluids. Guidelines recommend immediate transport to specialised burn centres when certain criteria are met. To date, there is still insufficient knowledge on the characteristics of prehospital emergency treatment. We sought to investigate the current practice and its potential effects on patient outcome.
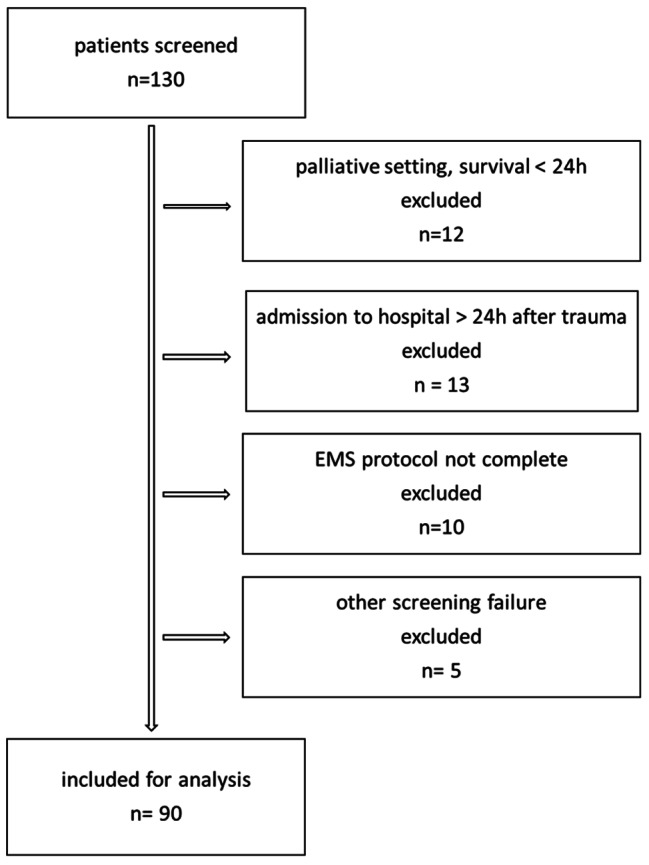
Methods: We conducted a single centre, retrospective cohort analysis of severely burned patients (total burned surface area > 20%), admitted to the Berlin burn centre between 2014 and 2019. The relevant data was extracted from Emergency Medical Service reports and digital patient charts for exploratory data analysis. Primary outcome was 28-day-mortality.
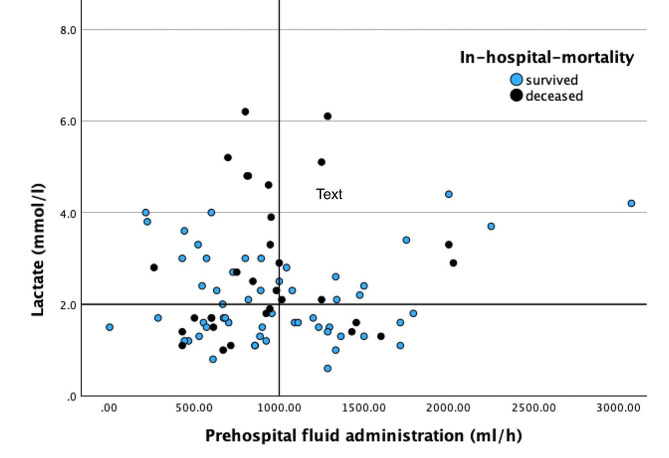
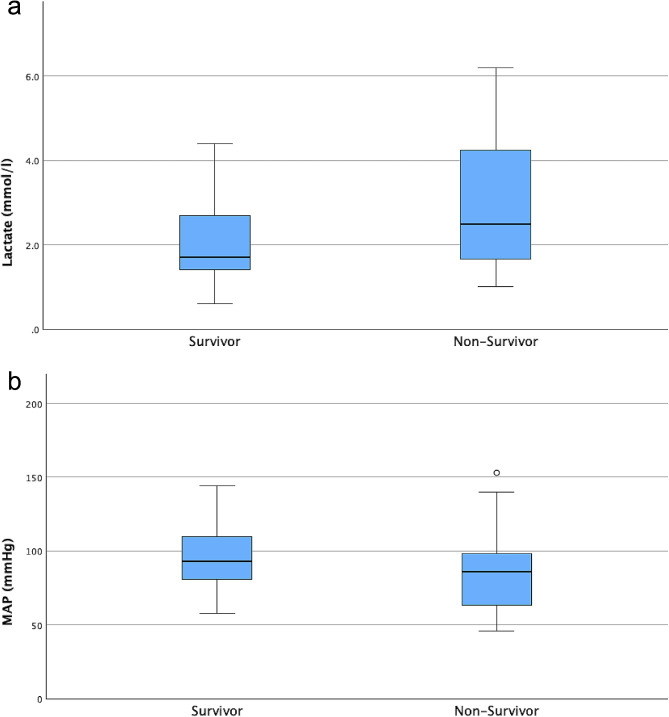
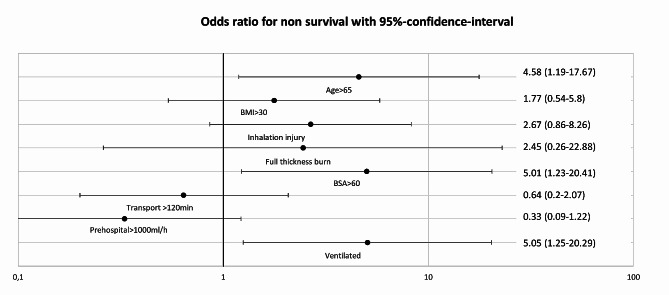
Results: Ninety patients (male/female 60/30, with a median age of 52 years [interquartile range, IQR 37-63], median total burned surface area 36% [IQR 25-51] and median body mass index 26.56 kg/m2 [IQR 22.86-30.86] were included. The median time from trauma to ED arrival was 1 h 45 min; within this time, on average 1961 ml of crystalloid fluid (0.48 ml/kg/%TBSA, IQR 0.32-0.86) was administered. Most patients received opioid-based analgesia. Times from trauma to ED arrival were longer for patients who were intubated. Neither excessive fluid treatment (> 1000 ml/h) nor transport times > 2 h was associated with higher mortality. A total of 31 patients (34,4%) died within the hospital stay. Multivariate regression analysis revealed that non-survival was linked to age > 65 years (odds ratio (OR) 3.5, 95% CI: 1.27-9.66), inhalation injury (OR 3.57, 95% CI: 1.36-9.36), burned surface area > 60% (OR 5.14, 95% CI 1.57-16.84) and prehospital intubation (5.38, 95% CI: 1.92-15.92).
Conclusion: We showed that severely burned patients frequently received excessive fluid administration prehospitally and that this was not associated with more hemodynamic stability or outcome. In our cohort, patients were frequently intubated prehospitally, which was associated with increased mortality rates. Further research and emergency medical staff training should focus on adequate fluid application and cautious decision-making on the risks and benefits of prehospital intubation.
Trial registration: German Clinical Trial Registry (ID: DRKS00033516).
Keywords: Advanced trauma care; Burn injury; Critical care; Emergency Medical Service; Fluid resuscitation; Prehospital airway management; Prehospital emergency care.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Smolle C, Cambiaso-Daniel J, Forbes AA, Wurzer P, Hundeshagen G, Branski LK et al. Recent trends in burn epidemiology worldwide: A systematic review. Burns. 2017 [cited 2024 Jan 12];43:249–57. https://linkinghub.elsevier.com/retrieve/pii/S0305417916302923 - PMC - PubMed
-
- Spanholtz TA, Theodorou P, Amini P, Spilker G. Severe Burn Injuries. Deutsches Ärzteblatt international. 2009 [cited 2024 Jan 16]; https://www.aerzteblatt.de/10.3238/arztebl.2009.0607 - PMC - PubMed
-
- AWMF. S2k-Leitlinie – Behandlung thermischer Verletzungen des Erwachsenen AWMF-Register-Nr.: 044 – 001. 2021 [cited 2024 Jan 16]. https://register.awmf.org/assets/guidelines/044-001l_S2k_Behandlung-ther...
-
- Allison K. Consensus on the prehospital approach to burns patient management. Emergency Medicine Journal. 2004 [cited 2024 Jan 16];21:112–4. https://emj.bmj.com/lookup/doi/10.1136/emj.2003.008789 - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
