

Clinical Presentation and Treatment Outcomes of Renal Medullary Angiitis in Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single-Center Case Series
- PMID: 39144476
- PMCID: PMC11324220
- DOI: 10.1159/000539553
Clinical Presentation and Treatment Outcomes of Renal Medullary Angiitis in Antineutrophil Cytoplasmic Antibody-Associated Vasculitis: A Single-Center Case Series
Abstract
Introduction: Antineutrophil cytoplasmic antibody-associated vasculitis (AAV) with renal involvement primarily affects the renal cortex and presents with key histopathologic findings of a pauci-immune necrotizing and crescentic glomerulonephritis. Infrequently reported and poorly characterized is renal medullary angiitis (RMA), a pathologic variant of AAV primarily involving the renal medulla. This study seeks to describe the presentation and treatment outcomes of RMA.
Methods: In this single-center cohort, renal pathology samples classified as AAV with renal involvement underwent secondary review to determine if they met histopathologic criteria for RMA. Demographic, clinical, and laboratory data were obtained via electronic medical record review. Descriptive statistical analysis was performed on key variables.
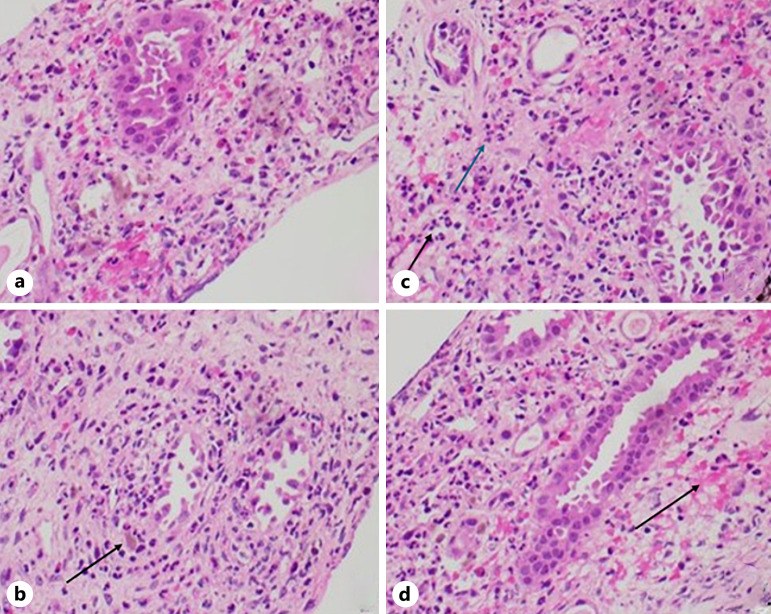
Results: Of the 136 kidney biopsy samples classified as AAV with renal involvement, histopathologic features of RMA were present in 13 cases. The mean (SD) age at the time of RMA diagnosis was 65 (19) years, and 54% were female. Most cases presented with extrarenal manifestations of disease. Initial median (IQR) estimated glomerular filtration rate and proteinuria on presentation were 16 (10-19) mL/min/1.73 m2 and 1,100 (687-2,437) mg, respectively. The primary histologic features were high degrees of interstitial inflammation comprised leukocytes, neutrophils, plasma cells, and eosinophils along with either interstitial hemorrhage or necrosis. All patients were treated with glucocorticoids in combination with either cyclophosphamide, rituximab, or mycophenolate. All patients achieved disease remission. During a median (IQR) follow-up of 42 (14-68) months, 1 patient reached ESKD and 1 patient died.
Conclusions: In this single-center case series, we identified the presence of RMA in 9.5% of AAV samples that underwent secondary review. RMA presented with severe impairment in renal function and multisystem disease. Standard of care immunosuppression for AAV was effective for remission induction in RMA. It remains unclear whether standard prognostication tools are useful in this population.
Keywords: Antineutrophil cytoplasmic antibody vasculitis; Outcomes; Renal medullary angiitis.
© 2024 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
Grant Kirby, Antonio Salas, Abdulrahman Alabdulsalam, and Alana Dasgupta have no conflicts of interest to declare. Duvuru Geetha is a consultant to Amgen, ChemoCentryx, Aurinia Inc., GSK, Calliditas, and Otsuka.
Figures
References
-
- Berden AE, Ferrario F, Hagen EC, Jayne DR, Jennette JC, Joh K, et al. Histopathologic classification of ANCA-associated glomerulonephritis. J Am Soc Nephrol. 2010;21(10):1628–36 Epub 2010 Jul 8. - PubMed
-
- Hendricks AR, Harris AA, Walker PD, Larsen CP. Renal medullary angiitis: a case series from a single institution. Hum Pathol. 2013;44(4):521–5 Epub 2012 Oct 15. - PubMed
-
- Brix SR, Noriega M, Tennstedt P, Vettorazzi E, Busch M, Nitschke M, et al. Development and validation of a renal risk score in ANCA-associated glomerulonephritis. Kidney Int. 2018;94(6):1177–88 Epub 2018 Oct 29. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous