

Interhospital transfer dynamics for patients with intracranial hemorrhage in Massachusetts
- PMID: 39144707
- PMCID: PMC11322084
- DOI: 10.3389/fneur.2024.1409713
Interhospital transfer dynamics for patients with intracranial hemorrhage in Massachusetts
Abstract
Introduction: Intracranial hemorrhages present across a spectrum of clinical phenotypes, with many patients transferred across hospitals to access higher levels of neurocritical care. We sought to characterize patient dispositions following intracranial hemorrhage and examine disparities associated with interhospital transfers.
Methods: Using the Healthcare Cost and Utilization Project database, we mapped and identified factors influencing the likelihood of patient transfers and receipt of specialist interventional procedures following intracranial hemorrhage.
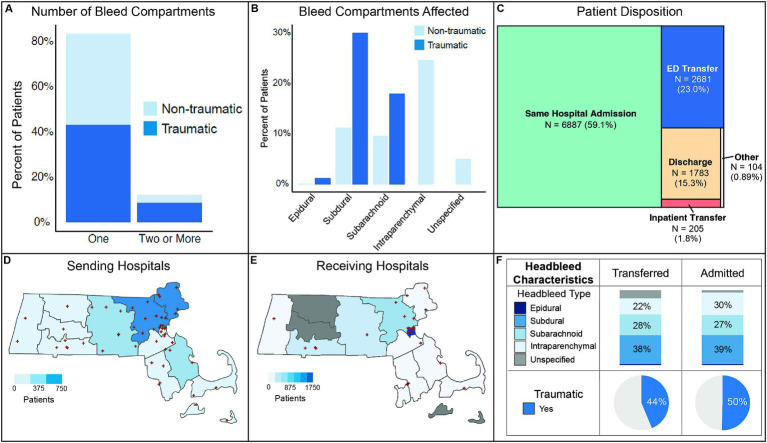
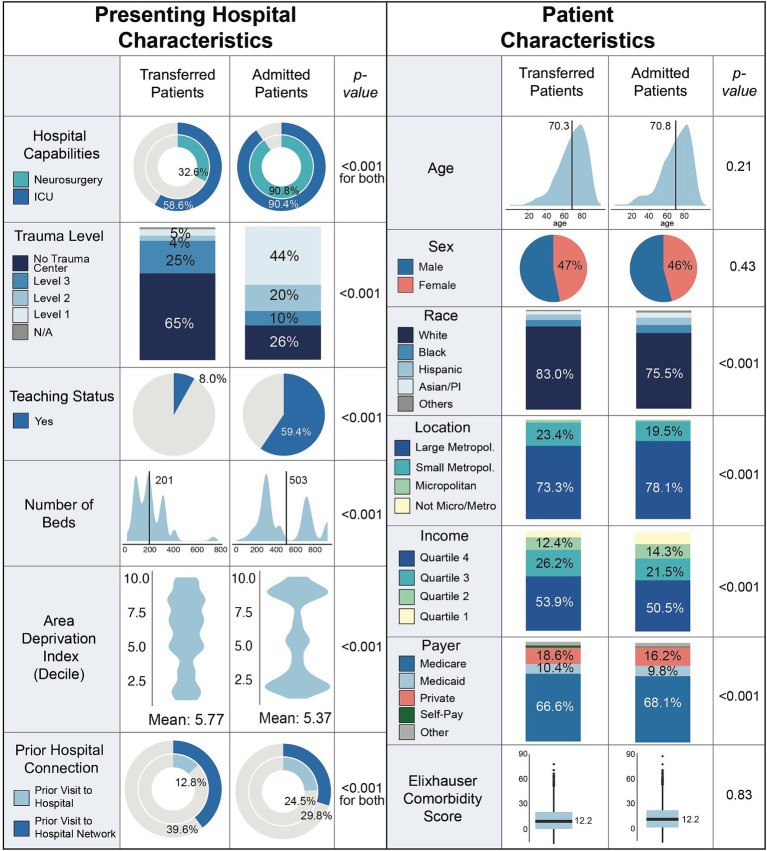
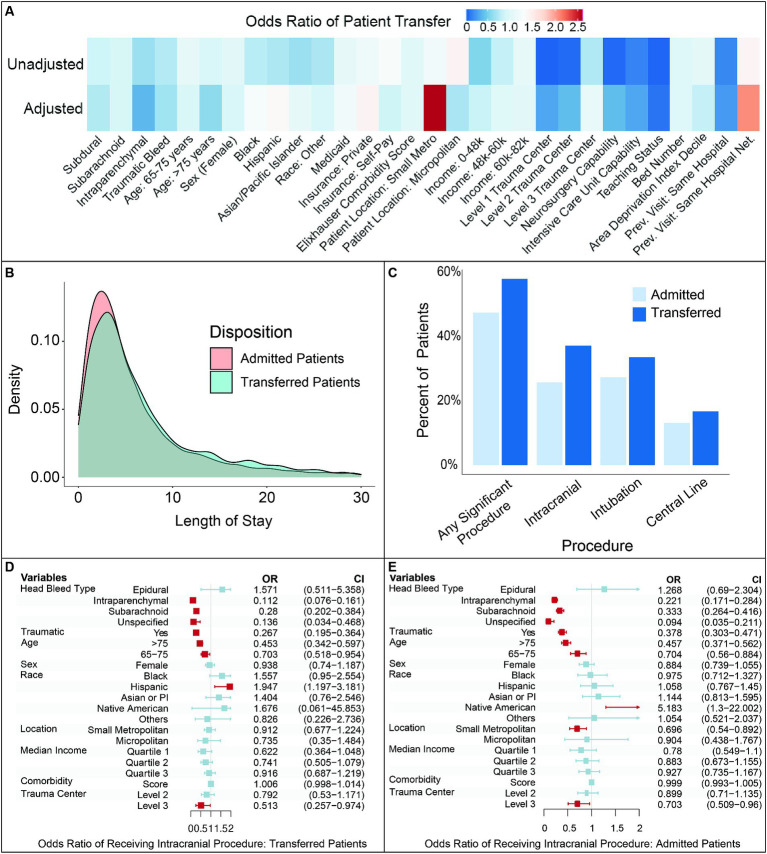
Results: Of 11,660 patients with intracranial hemorrhage, 59.4% had non-traumatic and 87.5% single compartment bleeds. After presentation, about a quarter of patients were transferred to another facility either directly from the ED (23.0%) or after inpatient admission (1.8%). On unadjusted analysis, patients who were white, in the upper income quartiles, with private insurance, or resided in suburban areas were more frequently transferred. After adjusting for patient-and hospital-level variables, younger and non-white patients had higher odds of transfer. Hospital capabilities, residence location, insurance status, and prior therapeutic relationship remained as transfer predictors. Transferred patients had a similar hospital length of stay compared to admitted patients, with 43.1% having no recorded surgical or specialist interventional procedure after transfer.
Discussion: Our analysis reveals opportunities for improvement in risk stratification guiding transfers, as well as structural challenges likely impacting transfer decisions.
Keywords: health infrastructure; healthcare systems; intracranial hemorrhage; patient transfers; socioeconomics.
Copyright © 2024 Patel, Tong, Molyneaux, Patel, Aziz-Sultan, Dhand and Bi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Dissecting patterns and predictors of interhospital transfers for patients with brain metastasis.J Neurosurg. 2023 Jul 14;140(1):27-37. doi: 10.3171/2023.5.JNS222922. Print 2024 Jan 1. J Neurosurg. 2023. PMID: 37486906 Free PMC article.
-
Trends in Interhospital Transfers and Mechanical Thrombectomy for United States Acute Ischemic Stroke Inpatients.J Stroke Cerebrovasc Dis. 2019 Apr;28(4):980-987. doi: 10.1016/j.jstrokecerebrovasdis.2018.12.018. Epub 2019 Jan 8. J Stroke Cerebrovasc Dis. 2019. PMID: 30630752
-
Opportunity to reduce transfer of patients with mild traumatic brain injury and intracranial hemorrhage to a Level 1 trauma center.Am J Emerg Med. 2017 Sep;35(9):1281-1284. doi: 10.1016/j.ajem.2017.03.071. Epub 2017 Mar 30. Am J Emerg Med. 2017. PMID: 28385479
-
National Trends in Transfer of Patients with Primary Intracerebral Hemorrhage: An Analysis of 12-Year Nationwide Data.J Stroke Cerebrovasc Dis. 2021 Dec;30(12):106116. doi: 10.1016/j.jstrokecerebrovasdis.2021.106116. Epub 2021 Sep 22. J Stroke Cerebrovasc Dis. 2021. PMID: 34562791
-
Relationship between insurance status and interhospital transfers among cancer patients in the United States.BMC Cancer. 2022 Jan 29;22(1):121. doi: 10.1186/s12885-022-09242-8. BMC Cancer. 2022. PMID: 35093015 Free PMC article.
Cited by
-
Bleeding-Related Hospitalizations Among Direct Oral Anticoagulant Users and Nonusers in Medicare Fee-For-Service: Variation in Prevalence, Burden, and Characteristics.Adv Ther. 2025 Jul 22. doi: 10.1007/s12325-025-03287-4. Online ahead of print. Adv Ther. 2025. PMID: 40694275
-
A visualization analysis of research on arterial compression hemostatic devices using VOSviewer and CiteSpace.Front Neurol. 2025 Mar 5;16:1540909. doi: 10.3389/fneur.2025.1540909. eCollection 2025. Front Neurol. 2025. PMID: 40109848 Free PMC article.
References
-
- Woo D, Comeau ME, Venema SU, Anderson CD, Flaherty M, Testai F, et al. . Risk factors associated with mortality and neurologic disability after intracerebral hemorrhage in a racially and ethnically diverse cohort. JAMA Netw Open. (2022) 5:e221103. doi: 10.1001/jamanetworkopen.2022.1103, PMID: - DOI - PMC - PubMed
-
- Greenberg SM, Ziai WC, Cordonnier C, Dowlatshahi D, Francis B, Goldstein JN, et al. . 2022 guideline for the Management of Patients with Spontaneous Intracerebral Hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke. (2022) 53:e282–361. doi: 10.1161/STR.0000000000000407, PMID: - DOI - PubMed
-
- Bako AT, Bambhroliya A, Meeks J, Pan A, Potter T, Ifejika N, et al. . National Trends in transfer of patients with primary intracerebral hemorrhage: an analysis of 12-year Nationwide data. J Stroke Cerebrovasc Dis. (2021) 30:106116. doi: 10.1016/j.jstrokecerebrovasdis.2021.106116, PMID: - DOI - PubMed
LinkOut - more resources
Full Text Sources