

Should Prophylactic Endotracheal Intubation Be Performed in Upper Gastrointestinal Bleeding?
- PMID: 39144893
- PMCID: PMC11323713
- DOI: 10.7759/cureus.64567
Should Prophylactic Endotracheal Intubation Be Performed in Upper Gastrointestinal Bleeding?
Abstract
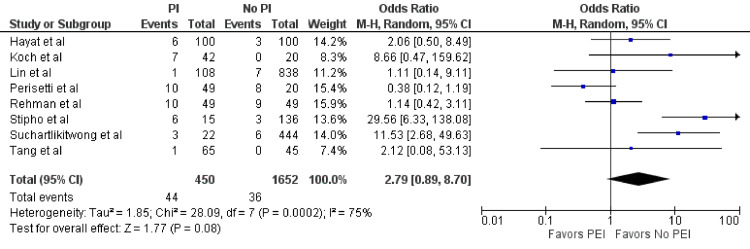
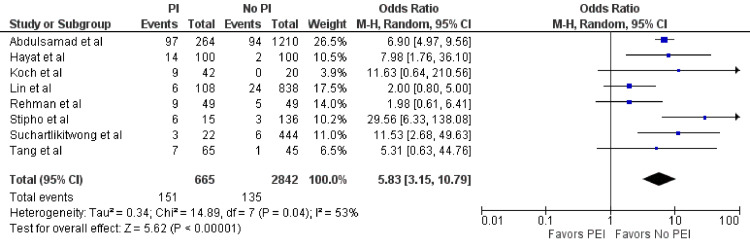
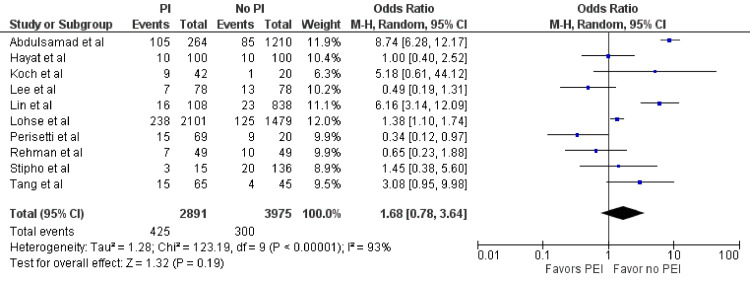
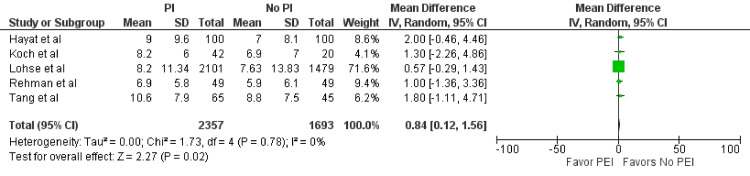
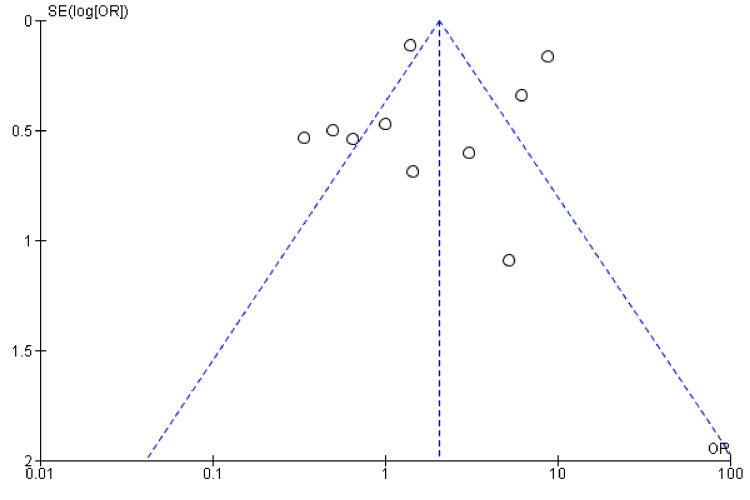
No consensus exists on the standard of intraoperative airway management approach to prevent endoscopy complications in acute gastrointestinal (GI) bleeding. Eight years after our initial meta-analysis, we reassessed the effect of prophylactic endotracheal intubation in acute GI bleeding in hospitalized patients. Multiple databases were reviewed in 2024, identifying 10 studies that compared prophylactic endotracheal intubation (PEI) versus no intubation in acute upper GI bleeding in hospitalized patients. Outcomes of interest included pneumonia, length of hospital stay, aspiration, and mortality. The odds ratio (OR) or mean difference (MD) using the random effects model was calculated for each outcome. In total, 11 studies (10 retrospective, one prospective) were included in the meta-analysis (n = 7,332). PEI demonstrated statistically significant higher odds of pneumonia (OR = 5.83; 95% confidence interval (CI) = 3.15-10.79; p < 0.01) and longer length of stays (MD = 0.84; 95% CI = 0.12-1.56; p = 0.02). However, mortality (OR = 1.68; 95% CI = 0.78-3.64; p = 0.19) and aspiration (OR = 2.79; 95% CI = 0.89-8.7; p = 0.08) were not statistically significant. PEI before esophagogastroduodenoscopy for hospitalized upper GI bleeding patients is associated with an increased incidence of pneumonia within 48 hours and prolonged hospitalization but no statistically significant increased risk of mortality or aspiration.
Keywords: bleeding; length of stay; meta-analysis; pneumonia; prophylactic intubation.
Copyright © 2024, Pasha et al.
Conflict of interest statement
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: Matthew Bechtold MD declare(s) personal fees from Medtrition. Advisory Board. Matthew Bechtold MD declare(s) personal fees from Nestle Nutrition Institute. Nutrition lectures. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Upper gastrointestinal bleeding: etiologies and management. Kamboj AK, Hoversten P, Leggett CL. Mayo Clin Proc. 2019;94:697–703. - PubMed
-
- Association of prophylactic endotracheal intubation in critically ill patients with upper GI bleeding and cardiopulmonary unplanned events. Hayat U, Lee PJ, Ullah H, Sarvepalli S, Lopez R, Vargo JJ. Gastrointest Endosc. 2017;86:500–509. - PubMed
-
- Anaesthesia care with and without tracheal intubation during emergency endoscopy for peptic ulcer bleeding: a population-based cohort study. Lohse N, Lundstrøm LH, Vestergaard TR, Risom M, Rosenstock SJ, Foss NB, Møller MH. Br J Anaesth. 2015;114:901–908. - PubMed
-
- Risk of aspiration pneumonia in suspected variceal hemorrhage: the value of prophylactic endotracheal intubation prior to endoscopy. Koch DG, Arguedas MR, Fallon MB. Dig Dis Sci. 2007;52:2225–2228. - PubMed
-
- Prophylactic endotracheal intubation prior to urgent endoscopy in patients with suspected variceal hemorrhage: an evaluation of outcomes and complications. Tang YM, Wang W. http://www.ghrnet.org/index.php/joghr/article/view/1968/2365 J Gastroenterol Hepatol Res. 2017;6:2324–2328.
Publication types
LinkOut - more resources
Full Text Sources