

Identification of Succinate Dehydrogenase Gene Variant Carriers by Blood Biomarkers
- PMID: 39145115
- PMCID: PMC11323779
- DOI: 10.1210/jendso/bvae142
Identification of Succinate Dehydrogenase Gene Variant Carriers by Blood Biomarkers
Abstract
Background: Carriers of germline pathogenic variants (PVs) in succinate dehydrogenase genes (SDHx) are at risk of developing tumors, including paragangliomas, gastrointestinal stromal tumors, and renal cell carcinomas. Early tumor detection is paramount for improved clinical outcome. Blood-based biomarkers could aid in identifying individuals with PVs early and provide functional evidence in patients with variants of unknown significance.
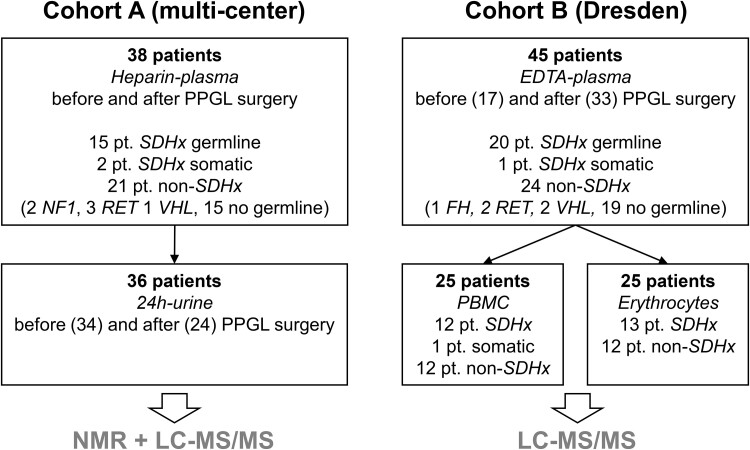
Methods: Blood plasma, urine, peripheral blood mononuclear cells, and erythrocytes from patients with and without SDHx PVs were investigated for central carbon metabolites. These were measured by liquid chromatography-tandem mass spectrometry and nuclear magnetic resonance spectroscopy and included among others, succinate, fumarate, α-ketoglutarate, and lactate.
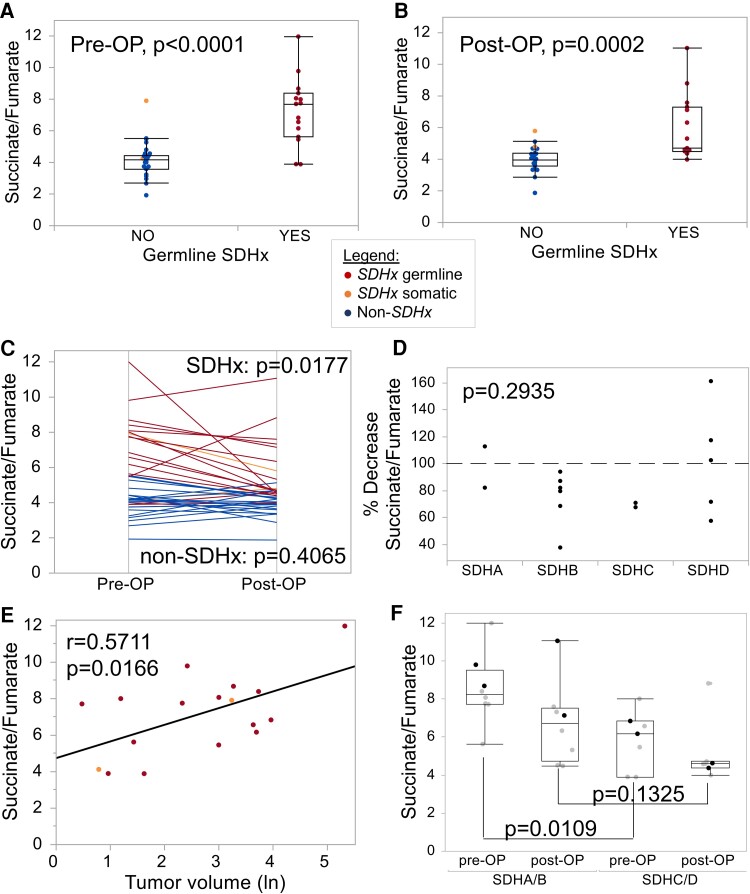
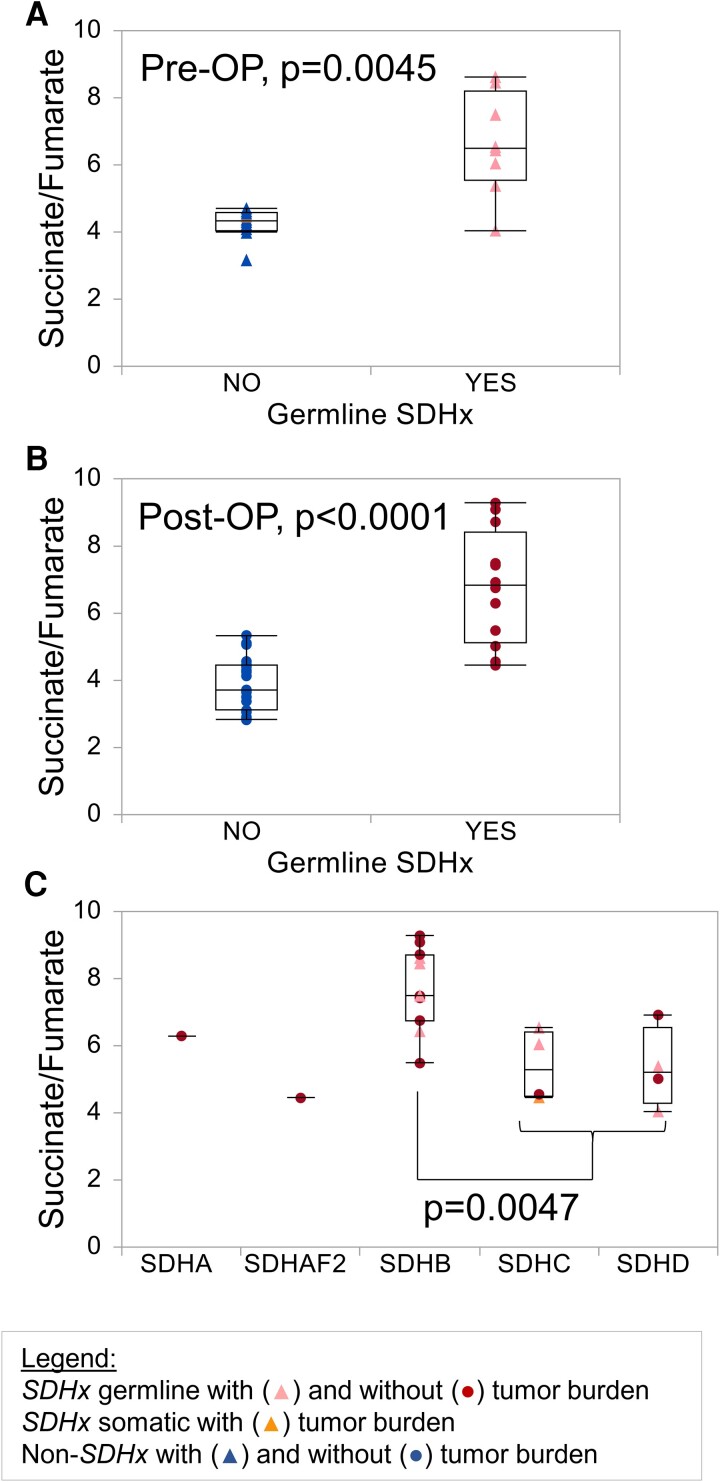
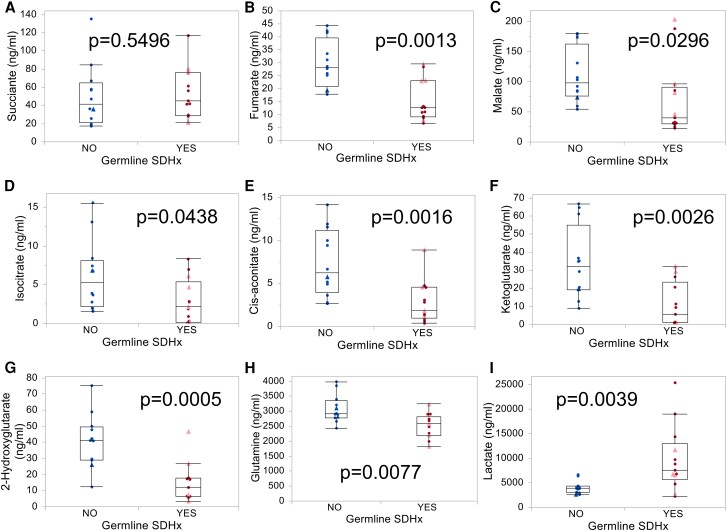
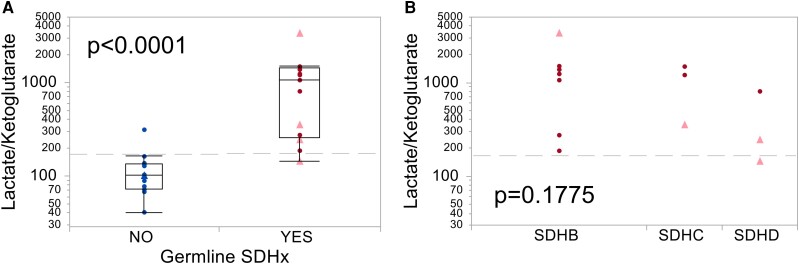
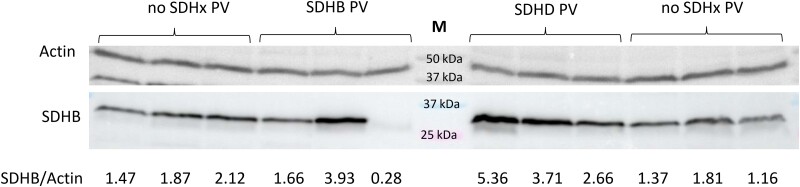
Results: Plasma succinate to fumarate ratios effectively distinguished tumor-bearing and asymptomatic patients with and without SDHx PV with promising diagnostic performance (areas under the receiver operating characteristic curve 0.86-0.95), although higher levels were noted in individuals with SDHB PV. Metabolites in urine and in peripheral blood mononuclear cell extracts were largely similar between groups. Erythrocytes showed strong metabolic alterations in patients with SDHx PV compared to controls, with 8 of 13 low-molecular organic acids being significantly different (P < .05). The lactate-α-ketoglutarate-ratio of erythrocytes identified individuals with SDHx PV equally well as plasma, with a sensitivity and specificity of 92% (AUC 0.97).
Conclusion: Blood biomarkers have been underutilized for identifying carriers of SDHx PV or to validate variants of unknown significance. Our findings advocate for further investigation into a combined approach involving plasma and erythrocytes for future diagnostic strategies.
Keywords: PBMC; blood plasma; erythrocytes; metabolism; succinate dehydrogenase gene variants; urine.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- MacFarlane J, Seong KC, Bisambar C, et al. A review of the tumour spectrum of germline succinate dehydrogenase gene mutations: beyond phaeochromocytoma and paraganglioma. Clin Endocrinol. 2020;93(5):528‐538. - PubMed
-
- Buffet A, Ben Aim L, Leboulleux S, et al. Positive impact of genetic test on the management and outcome of patients with paraganglioma and/or pheochromocytoma. J Clin Endocrinol Metab. 2019;104(4):1109‐1118. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials