

Perfusion Abnormalities on 24-Hour Perfusion Imaging in Patients With Complete Endovascular Reperfusion
- PMID: 39145382
- PMCID: PMC11346709
- DOI: 10.1161/STROKEAHA.124.047441
Perfusion Abnormalities on 24-Hour Perfusion Imaging in Patients With Complete Endovascular Reperfusion
Abstract
Background: Perfusion abnormalities in the infarct and salvaged penumbra have been proposed as a potential reason for poor clinical outcome (modified Rankin Scale score >2) despite complete angiographic reperfusion (Thrombolysis in Cerebral Infarction [TICI3]). In this study, we aimed to identify different microvascular perfusion patterns and their association with clinical outcomes among TICI3 patients.
Methods: University Hospital Bern's stroke registry of all patients between February 2015 and December 2021. Macrovascular reperfusion was graded using the TICI scale. Microvascular reperfusion status was evaluated within the infarct area on cerebral blood volume and cerebral blood flow perfusion maps obtained 24-hour postintervention. Primary outcome was functional independence (90-day modified Rankin Scale score 0-2) evaluated with the logistic regression analysis adjusted for age, sex, and 24-hour infarct volume from follow-up imaging.
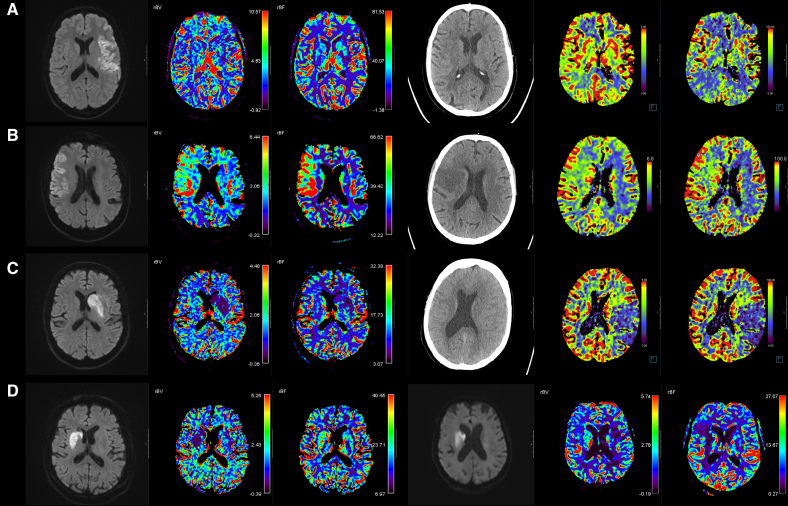
Results: Based on microvascular perfusion findings, the entire cohort (N=248) was stratified into one of the 4 clusters: (1) normoperfusion (no perfusion abnormalities; n=143/248); (2) hyperperfusion (hyperperfusion on both cerebral blood volume and cerebral blood flow; n=54/248); (3) hypoperfusion (hypoperfusion on both cerebral blood volume and cerebral blood flow; n=14/248); and (4) mixed (discrepant findings, eg, cerebral blood volume hypoperfusion and cerebral blood flow hyperperfusion; n=37/248). Compared with the normoperfusion cluster, patients in the hypoperfusion cluster were less likely to achieve functional independence (adjusted odds ratio, 0.3 [95% CI, 0.1-0.9]), while patients in the hyperperfusion cluster tended to have better outcomes (adjusted odds ratio, 3.3 [95% CI, 1.3-8.8]).
Conclusions: In around half of TICI3 patients, perfusion abnormalities on the microvascular level can be observed. Microvascular hypoperfusion, despite complete macrovascular reperfusion, is rare but may explain the poor clinical course among some TICI3 patients, while a detrimental effect of hyperperfusion after reperfusion could not be confirmed.
Keywords: cerebrovascular circulation; perfusion; reperfusion; stroke; thrombolytic therapy.
Conflict of interest statement
Dr Mujanovic reports financial support from the Swiss National Science Foundation (fees paid to institution). Dr Piechowiak reports research grants from the Swiss National Science Foundation supporting the PASTA trial (Paediatric Arteriopathy Steroid Aspirin). Dr Dobrocky reports Microvention consultancy. Dr Seiffge reports grants from AstraZeneca and compensation from AstraZeneca for consultant services. Dr Goeldlin reports grants from the Swiss Academy of Medical Sciences, Gottfried und Julia Bangerter-Rhyner-Stiftung, Mittelbauvereinigung der Universität Bern, European Stroke Organization, Swiss Stroke Society, and Inselspital Bern University Hospital; and travel support from the European Academy of Neurology and Pfizer Switzerland; all outside the submitted study. Dr Arnold reports compensation from Novo Nordisk, Covidien, Medtronic, Boehringer Ingelheim, Amgen, AstraZeneca, Bayer, Bristol Myers Squibb, Covidien, Daiichi Sankyo, Novartis, Sanofi, and Pfizer for consultant services. Dr Gralla reports compensation from Johnson & Johnson Health Care Systems Inc for consultant services and compensation from Medtronic USA Inc for other services. Dr Mistry reports grants from the National Institute of Neurological Disorders and Stroke, Society of Vascular and Interventional Neurology, National Institutes of Health, and Patient-Centered Outcomes Research Institute; compensation from American Heart Association, RAPID AI, the American Heart Association, and AbbVie for consultant services; employment by the University of Cincinnati; compensation from Translational Sciences and Silver Creek Pharmaceuticals Inc for other services. Dr Fischer reports research support of the Swiss National Science Foundation and the Swiss Heart Foundation/Schweizerische Herzstiftung; PI of the ELAN trial (Early Versus Late Initiation of Direct Oral Anticoagulants in Post-Ischaemic Stroke Patients With Atrial Fibrillation), Co-PI of the DISTAL (Endovascular Therapy Plus Best Medical Treatment [BMT] Versus BMT Alone for MedIum Vessel Occlusion Stroke), TECNO (Safety and Efficacy of Intra-Arterial Tenecteplase for Non-Complete Reperfusion of Intracranial Occlusions), SWIFT DIRECT (Solitaire With the Intention for Thrombectomy Plus Intravenous t-PA Versus DIRECT Solitaire Stent-Retriever Thrombectomy in Acute Anterior Circulation Stroke), SWITCH (Swiss Trial of Decompressive Craniectomy Versus Best Medical Treatment of Spontaneous Supratentorial Intracerebral Hemorrhage), ELAPSE (Early Closure of Left Atrial Appendage for Patients With Atrial Fibrillation and Ischemic Stroke Despite Anticoagulation Therapy) and ICARUS (Inflammatory Factors After Acute Ischemic Stroke) trials; Steering committee member of the DO_IT trial; research grants from Medtronic (BEYOND SWIFT, SWIFT DIRECT), from Stryker, Rapid medical, Penumbra, Medtronic and phenox Inc (DISTAL), and from Boehringer Ingelheim (TECNO), whereas all fees were paid to the institution; consultancies for Medtronic, Stryker, and CSL Behring (fees paid to institution); participation in an advisory board for AstraZeneca (former Alexion/Portola), Boehringer Ingelheim, Biogen (expert witness services), AbbVie, and Acthera (fees paid to institution); member of a clinical event committee of the COATING study ([Coating to Optimize Aneurysm Treatment in the New Flow Diverter Generation]; Phenox) and member of the data and safety monitoring committee of the TITAN (Thrombectomy in Tandem Lesion), LATE_MT (Large Artery Occlusion Treated in Extended Time With Mechanical Thrombectomy), and IN EXTREMIS LASTE (Large Stroke Therapy Evaluation) trials; president of the Swiss Neurological Society, president-elect of the European Stroke Organization. Dr Wegener reports support by the Swiss National Science Foundation, the Universität Zürich Clinical Research Priority Program stroke, the Swiss Heart Foundation, the Zurich Neuroscience Center, the Baugarten Foundation, Koetser Foundation, Hartmann-Müller Foundation, and Olga-Mayenfish Foundation; speaker honoraria from Amgen, Springer, Teva Pharma, ADVISIS-AG, Forum für medizinische Fortbildung, Astra Zeneca, and a consultancy fee from Bayer and Novartis; all outside this study. Dr Kaesmacher reports Microvention consultancy within the frame work of a corelab, financial support from Medtronic for the BEYOND SWIFT registry and SWIFT DIRECT trial; medication supply support from Boheringer-Ingelheim for the TECNO trial, a research agreement with Siemens Healthineers regarding flat panel perfusion imaging, and research grants from the Swiss National Science Foundation supporting the TECNO trial, the Swiss Academy of Medical Sciences supporting MRI research, and the Swiss Heart Foundation supporting cardiac MRI in the etiological work-up of stroke patients and grants from Gottfried und Julia Bangerter-Rhyner-Stiftung. All fees are paid to the institutions. The other authors report no conflicts.
Figures

References
-
- Turc G, Bhogal P, Fischer U, Khatri P, Lobotesis K, Mazighi M, Schellinger PD, Toni D, De Vries J, White P, et al. . European Stroke Organisation (ESO) - European Society for Minimally Invasive Neurological Therapy (ESMINT) Guidelines on mechanical thrombectomy in acute ischemic stroke. J Neurointerv Surg. 2019;15:1–30. doi: 10.1136/neurintsurg-2018-014569 - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, et al. ; on behalf of the American Heart Association Stroke Council. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50;e344–e418. doi: 10.1161/STR.0000000000000211 - PubMed
-
- Majoie CB, Cavalcante F, Gralla J, Yang P, Kaesmacher J, Treurniet KM, Kappelhof M, Yan B, Suzuki K, Zhang Y, et al. ; IRIS Collaborators. Value of intravenous thrombolysis in endovascular treatment for large-vessel anterior circulation stroke: individual participant data meta-analysis of six randomised trials. Lancet. 2023;402:965–974. doi: 10.1016/S0140-6736(23)01142-X - PubMed
-
- Meinel TR, Lerch C, Fischer U, Beyeler M, Mujanovic A, Kurmann C, Siepen B, Scutelnic A, Müller M, Goeldlin M, et al. . Multivariable prediction model for futile recanalization therapies in patients with acute ischemic stroke. Neurology. 2022;99:e1009–e1018. doi: 10.1212/WNL.0000000000200815 - PMC - PubMed
-
- Van Kranendonk KR, Treurniet KM, Boers AMM, Berkhemer OA, Van Den Berg LA, Chalos V, Lingsma HF, Van Zwam WH, Van Der Lugt A, Van Oostenbrugge RJ, et al. ; MR CLEAN Investigators. Hemorrhagic transformation is associated with poor functional outcome in patients with acute ischemic stroke due to a large vessel occlusion. J Neurointerv Surg. 2019;11:464–468. doi: 10.1136/neurintsurg-2018-014141 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
