

Stress and substance use disorders: risk, relapse, and treatment outcomes
- PMID: 39145454
- PMCID: PMC11324296
- DOI: 10.1172/JCI172883
Stress and substance use disorders: risk, relapse, and treatment outcomes
Abstract
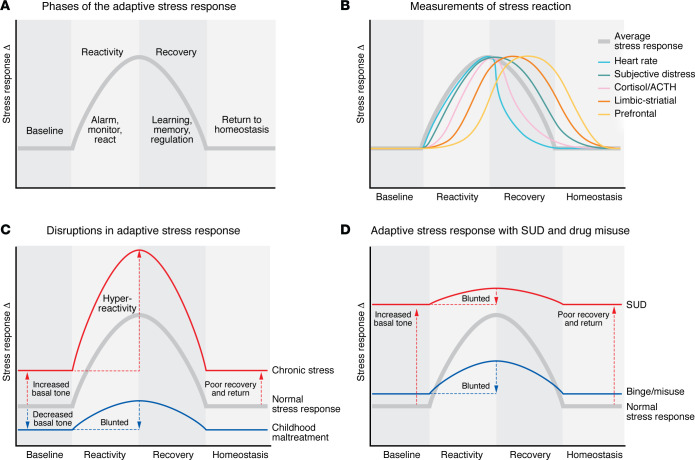
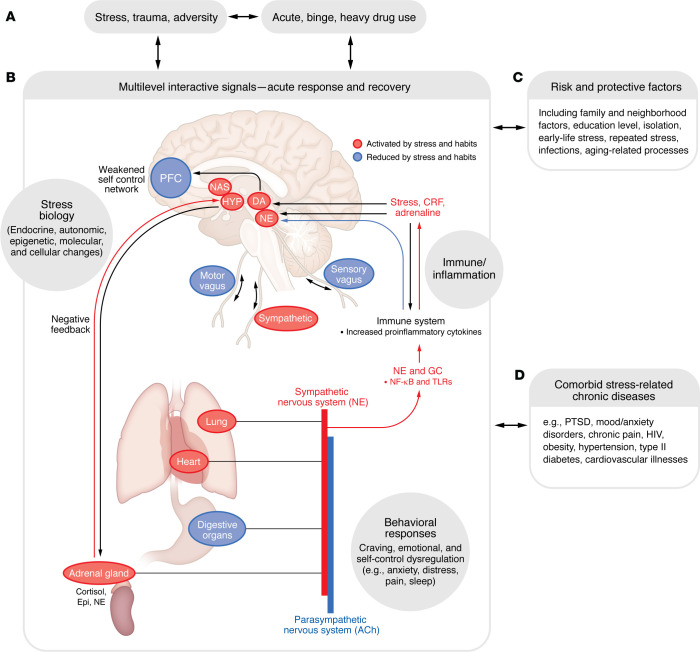
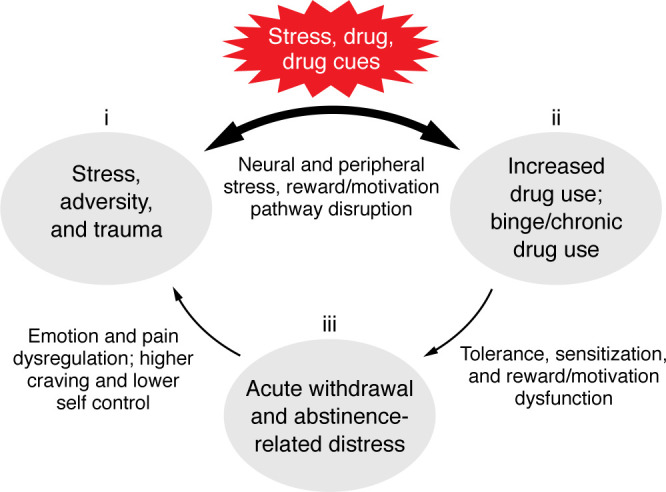
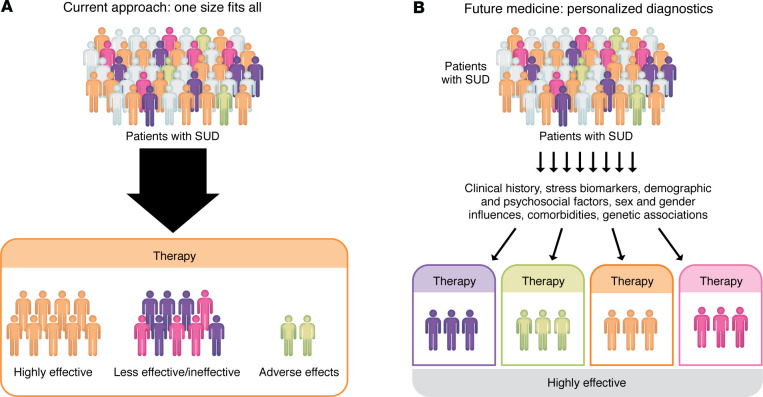
Stress has long been associated with substance misuse and substance use disorders (SUDs). The past two decades have seen a surge in research aimed at understanding the underlying mechanisms driving this association. This Review introduces a multilevel "adaptive stress response" framework, encompassing a stress baseline, acute reaction, and recovery with return-to-homeostasis phase that occurs at varying response times and across domains of analysis. It also discusses evidence showing the disruption of this adaptive stress response in the context of chronic and repeated stressors, trauma, adverse social and drug-related environments, as well as with acute and chronic drug misuse and with drug withdrawal and abstinence sequelae. Subjective, cognitive, peripheral, and neurobiological disruptions in the adaptive stress response phases and their link to inflexible, maladaptive coping; increased craving; relapse risk; and maintenance of drug intake are also presented. Finally, the prevention and treatment implications of targeting this "stress pathophysiology of addiction" are discussed, along with specific aspects that may be targeted in intervention development to rescue stress-related alterations in drug motivation and to improve SUD treatment outcomes.
Conflict of interest statement
Figures
References
-
- Carver CS, Scheier MF, eds. On the Self-Regulation of Behavior. Cambridge University Press; 2001.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
