

Risk willingness in multiple system atrophy and Parkinson's disease understanding patient preferences
- PMID: 39147806
- PMCID: PMC11327309
- DOI: 10.1038/s41531-024-00764-5
Risk willingness in multiple system atrophy and Parkinson's disease understanding patient preferences
Abstract
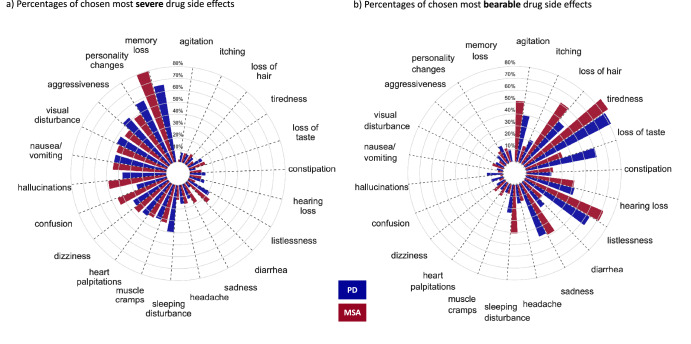
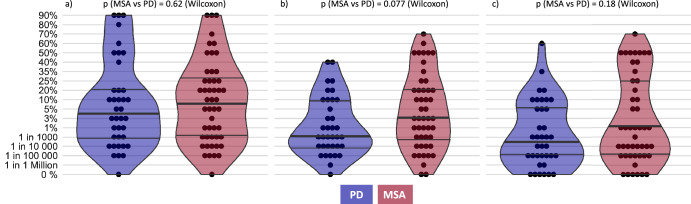
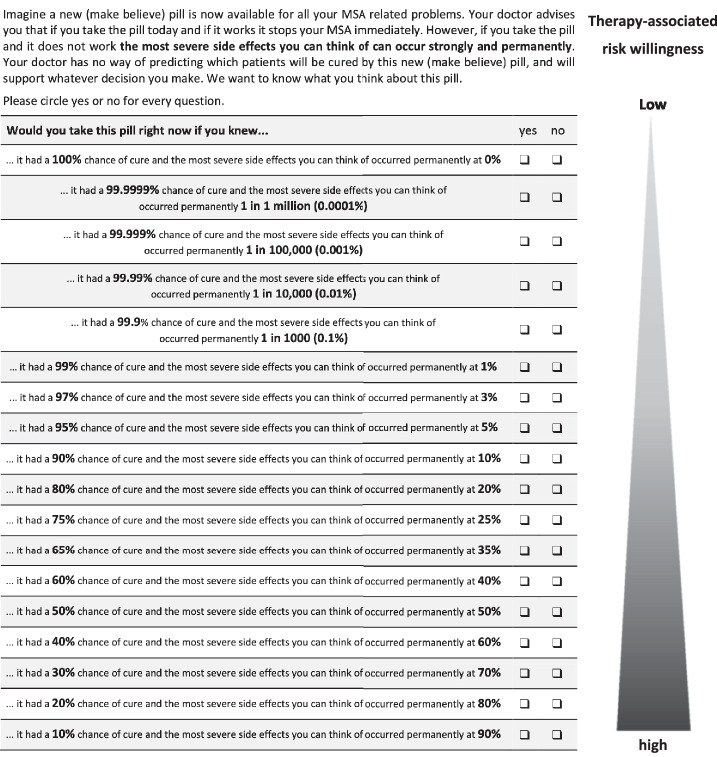
Disease-modifying therapeutics in the α-synucleinopathies multiple system atrophy (MSA) and Parkinson's Disease (PD) are in early phases of clinical testing. Involving patients' preferences including therapy-associated risk willingness in initial stages of therapy development has been increasingly pursued in regulatory approval processes. In our study with 49 MSA and 38 PD patients, therapy-associated risk willingness was quantified using validated standard gamble scenarios for varying severities of potential drug or surgical side effects. Demonstrating a non-gaussian distribution, risk willingness varied markedly within, and between groups. MSA patients accepted a median 1% risk [interquartile range: 0.001-25%] of sudden death for a 99% [interquartile range: 99.999-75%] chance of cure, while PD patients reported a median 0.055% risk [interquartile range: 0.001-5%]. Contrary to our hypothesis, a considerable proportion of MSA patients, despite their substantially impaired quality of life, were not willing to accept increased therapy-associated risks. Satisfaction with life situation, emotional, and nonmotor disease burden were associated with MSA patients' risk willingness in contrast to PD patients, for whom age, and disease duration were associated factors. An individual approach towards MSA and PD patients is crucial as direct inference from disease (stage) to therapy-associated risk willingness is not feasible. Such studies may be considered by regulatory agencies in their approval processes assisting with the weighting of safety aspects in a patient-centric manner. A systematic quantitative assessment of patients' risk willingness and associated features may assist physicians in conducting individual consultations with patients who have MSA or PD by facilitating communication of risks and benefits of a treatment option.
© 2024. The Author(s).
Conflict of interest statement
K.P. has been supported by the “Rostock Academy of Science” (RAS). I.C. has received honoraria for presentations/advisory boards from Abbvie, Stadapharm, BIAL, Zambon, Desitin, Georg Thieme Verlag KG, and Springer Verlag. C.P. is inventor in a patent “Oral Phenylbutyrate for Treatment of Human 4-Repeat Tauopathies” (EP 23 156 122.6) filed by LMU Munich. M.B. received funding from Europäischer Fonds für regionale Entwicklung (EFRE) and speaker fees from Novartis and Idorsia. A.H. has received funding from the European Social Fonds, the Federal Ministry of Education and Research and the Hermann und Lilly Schilling-Stiftung für medizinische Forschung im Stifterverband. He has received honoraria for presentations/advisory boards/ from Amylyx and IFT Pharma. He has received royalties from Elsevier Press and Kohlhammer. J.L. reports speaker fees from Bayer Vital, Biogen, EISAI, TEVA, and Roche, consulting fees from Axon Neuroscience and Biogen, author fees from Thieme medical publishers and W. Kohlhammer GmbH medical publishers and is inventor in a patent “Oral Phenylbutyrate for Treatment of Human 4-Repeat Tauopathies” (EP 23 156 122.6) filed by LMU Munich. In addition, he reports compensation for serving as chief medical officer for MODAG GmbH, is beneficiary of the phantom share program of MODAG GmbH and is inventor in a patent “Pharmaceutical Composition and Methods of Use” (EP 22 159 408.8) filed by MODAG GmbH, all activities outside the submitted work. A.G. reports employment by and being a shareholder of MODAG GmbH. In addition, he is inventor in a patent “water-soluble derivatives of 3,5-diphelyl-diazole compounds” (PCT EP 16/081084, etc.) licensed to MODAG GmbH, and a patent “new drugs for inhibiting aggregation of proteins involved in disease linked to protein aggregation and/or neurodegenerative diseases” (EP 2307381 etc.), which includes the compound anle138b, licensed to MODAG GmbH. W.H.O. reports grants from ParkinsonFonds Deutschland, grants from Michael J Fox Foundation, grants from Deutsche Forschungsgemeinschaft (DFG), all unrelated to the study during its conduct; speaker or consulting fees from Abbvie, Adamas, Lario Therapeutics, MODAG, Novartis, Stada Pharma and UCB all outside the submitted work. W.H.O. is Hertie-Senior-Research Professor supported by the Charitable Hertie-Foundation, Frankfurt/Main, Germany. All other authors declare no Competing Financial or Non-Financial Interests.
Figures

References
LinkOut - more resources
Full Text Sources
