

DNA liquid biopsy-based prediction of cancer-associated venous thromboembolism
- PMID: 39147831
- PMCID: PMC11405286
- DOI: 10.1038/s41591-024-03195-0
DNA liquid biopsy-based prediction of cancer-associated venous thromboembolism
Abstract
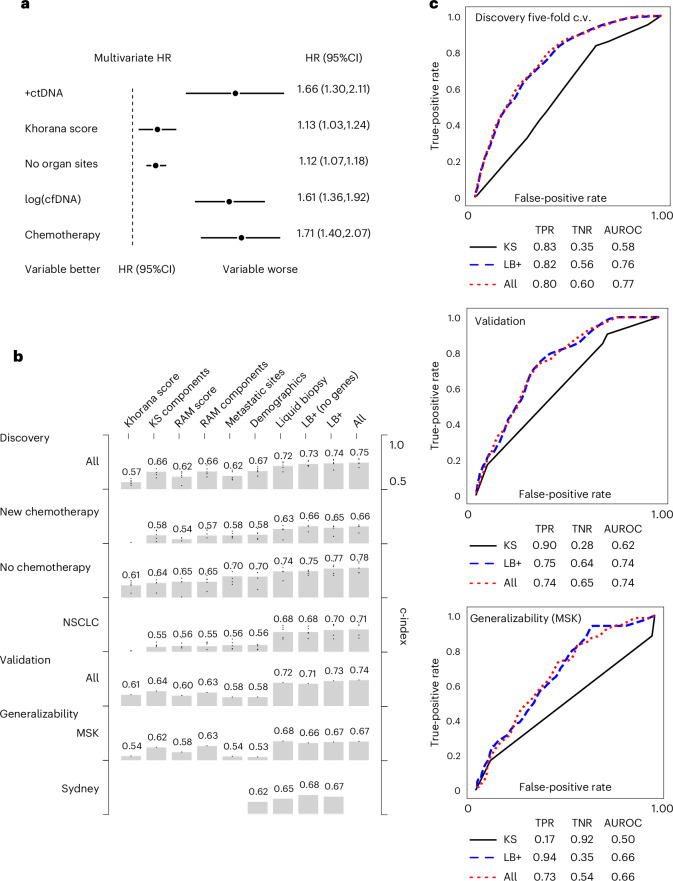
Cancer-associated venous thromboembolism (VTE) is a major source of oncologic cost, morbidity and mortality. Identifying high-risk patients for prophylactic anticoagulation is challenging and adds to clinician burden. Circulating tumor DNA (ctDNA) sequencing assays ('liquid biopsies') are widely implemented, but their utility for VTE prognostication is unknown. Here we analyzed three plasma sequencing cohorts: a pan-cancer discovery cohort of 4,141 patients with non-small cell lung cancer (NSCLC) or breast, pancreatic and other cancers; a prospective validation cohort consisting of 1,426 patients with the same cancer types; and an international generalizability cohort of 463 patients with advanced NSCLC. ctDNA detection was associated with VTE independent of clinical and radiographic features. A machine learning model trained on liquid biopsy data outperformed previous risk scores (discovery, validation and generalizability c-indices 0.74, 0.73 and 0.67, respectively, versus 0.57, 0.61 and 0.54 for the Khorana score). In real-world data, anticoagulation was associated with lower VTE rates if ctDNA was detected (n = 2,522, adjusted hazard ratio (HR) = 0.50, 95% confidence interval (CI): 0.30-0.81); ctDNA- patients (n = 1,619) did not benefit from anticoagulation (adjusted HR = 0.89, 95% CI: 0.40-2.0). These results provide preliminary evidence that liquid biopsies may improve VTE risk stratification in addition to clinical parameters. Interventional, randomized prospective studies are needed to confirm the clinical utility of liquid biopsies for guiding anticoagulation in patients with cancer.
© 2024. The Author(s).
Conflict of interest statement
J.J. has a patent licensed by MDSeq, Inc. J.G. is a former employee of Agilent Technologies and a current employee of NeoGenomics. J.H. and K.G. are current employees of Agilent Technologies. M.E.A. has consulted for Janssen Global Services, Bristol Myers Squibb, AstraZeneca, Roche and Biocartis and has participated in speaker’s bureau activities for Biocartis, Invivoscribe, Physiciansʼ Education Resource, PeerView Institute for Medical Education, Clinical Care Options and RMEI Medical Education. N.P. has received honoraria from Boehringer Ingelheim, Merck Sharp & Dohme, Merck, Bristol Myers Squibb, AstraZeneca, Takeda, Pfizer, Roche, Novartis, Ipsen and Bayer and received research funding from Bayer, Pfizer and Roche. S.P.S. holds equity in Canesia Health, Inc. P.R. has received research funding from GRAIL, Illumina, Novartis, Epic Sciences and ArcherDx and served as a consultant for Novartis, Foundation Medicine, AstraZeneca, Epic Sciences, Inivata, Natera and Tempus. J.S.R.-F. is a current employee of AstraZeneca; has served as a consultant for Goldman Sachs, Paige.AI and REPARE Therapeutics; and has served as an advisor for Roche, Genentech, Roche Tissue Diagnostics, Ventana, Novartis, InVicro, GRAIL, Goldman Sachs, Paige.AI and Volition RX. M.L. has received honoraria from Merck, AstraZeneca, Bristol Myers Squibb, Blueprint Medicines, Janssen Pharmaceuticals, Takeda Pharmaceuticals, Lilly Oncology, LOXO Oncology, Bayer, ADC Therapeutics, Riken Genesis and Paige.AI and research funding from LOXO Oncology, Merus and Helsinn Therapeutics. J.Z. has served as a consultant for Calyx, Sanofi, CSL Behring, Janssen, Sanofi, CSL and Parexel and received research funding from Incyte Corporation and QUercegen and honoraria from Pfizer/Bristol Myers Squibb, Portola and Daiichi. M.F.B. has consulted for PetDx and Eli Lilly and received research funding from GRAIL. B.T.L. has received research funding from Amgen, Genentech, AstraZeneca, Daiichi Sankyo, Eli Lilly, Illumina, GRAIL, Guardant Health, Hengrui Therapeutics, MORE Health and Bolt Biotherapeutics. S.M. has served as a consultant for Janssen Pharmaceuticals; is developing a licensing agreement with Superbio.ai, Inc. for NLP software featured in this paper; is the principal owner of Daboia Consulting, LLC; and has a US patent application for PINES. J.J., B.T.L. and S.M. have applied for a US patent related to the research in this paper. The other authors declare no competing interests.
Figures










References
-
- Agnelli, G. et al. Nadroparin for the prevention of thromboembolic events in ambulatory patients with metastatic or locally advanced solid cancer receiving chemotherapy: a randomised, placebo-controlled, double-blind study. Lancet Oncol.10, 943–949 (2009). 10.1016/S1470-2045(09)70232-3 - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
