

Population Pharmacokinetics and Target Attainment of Allopurinol and Oxypurinol Before, During, and After Cardiac Surgery with Cardiopulmonary Bypass in Neonates with Critical Congenital Heart Disease
- PMID: 39147988
- PMCID: PMC11343829
- DOI: 10.1007/s40262-024-01401-3
Population Pharmacokinetics and Target Attainment of Allopurinol and Oxypurinol Before, During, and After Cardiac Surgery with Cardiopulmonary Bypass in Neonates with Critical Congenital Heart Disease
Abstract
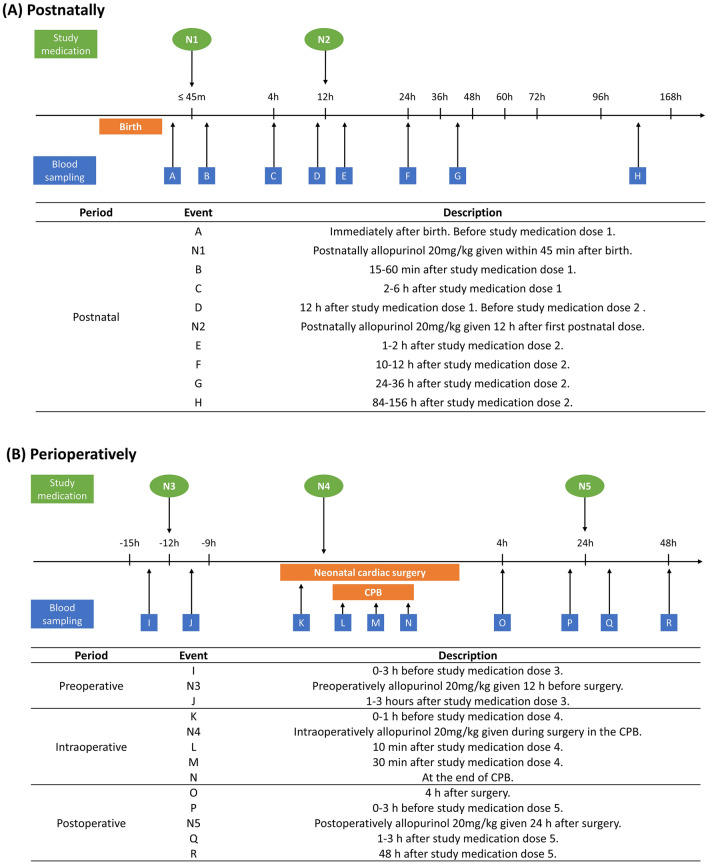
Background: The CRUCIAL trial (NCT04217421) is investigating the effect of postnatal and perioperative administration of allopurinol on postoperative brain injury in neonates with critical congenital heart disease (CCHD) undergoing cardiac surgery with cardiopulmonary bypass (CPB) shortly after birth.
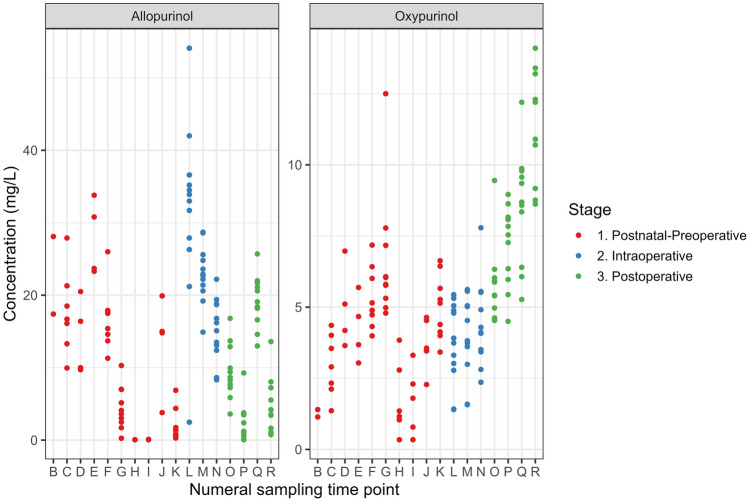
Objective: This study aimed to characterize the pharmacokinetics (PK) of allopurinol and oxypurinol during the preoperative, intraoperative, and postoperative phases in this population, and to evaluate target attainment of the current dosing strategy.
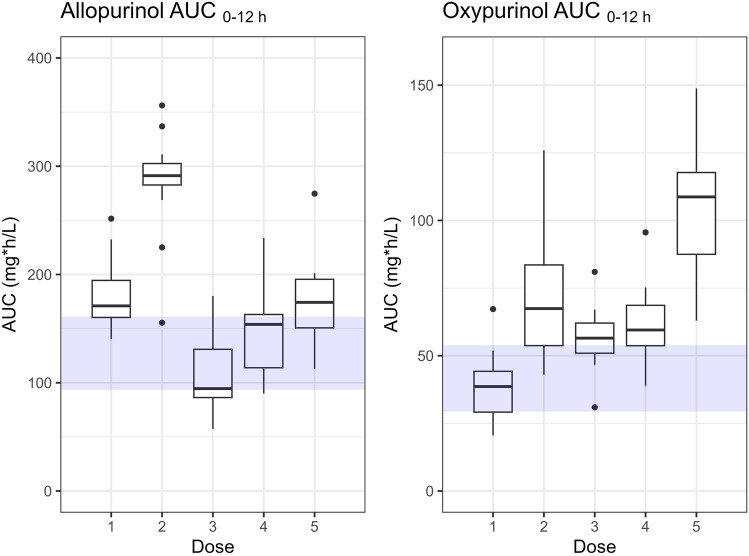
Methods: Nonlinear mixed-effects modeling was used to develop population PK models in 14 neonates from the CRUCIAL trial who received up to five intravenous allopurinol administrations throughout the postnatal and perioperative periods. Target attainment was defined as achieving an allopurinol concentration >2 mg/L in at least two-thirds of the patients during the first 24 h after birth and between the start and 36 h after cardiac surgery with CPB.
Results: A two-compartment model for allopurinol was connected to a one-compartment model for oxypurinol with an auto-inhibition effect on the conversion, which best described the PK. In a typical neonate weighing 3.5 kg who underwent cardiac surgery at a postnatal age (PNA) of 5.6 days, the clearance (CL) of allopurinol and oxypurinol at birth was 0.95 L/h (95% confidence interval 0.75-1.2) and 0.21 L/h (0.17-0.27), respectively, which subsequently increased with PNA to 2.97 L/h and 0.41 L/h, respectively, before CPB. During CPB, allopurinol and oxypurinol CL decreased to 1.38 L/h (0.9-1.87) and 0.12 L/h (0.05-0.22), respectively. Post-CPB, allopurinol CL increased to 2.21 L/h (1.74-2.83), while oxypurinol CL dropped to 0.05 L/h (0.01-0.1). Target attainment was 100%, 53.8%, and 100% at 24 h postnatally, 24 h after the start of CPB, and 36 h after the end of cardiac surgery, respectively. The combined concentrations of allopurinol and oxypurinol maintained ≥ 90% inhibition of xanthine oxidase (IC90XO) throughout the postnatal and perioperative period.
Conclusions: The minimal target concentration of allopurinol was not achieved at every predefined time interval in the CRUCIAL trial; however, the dosing strategy used was deemed adequate, since it yielded concentrations well exceeding the IC90XO. The decreased CL of both compounds during CPB suggests influence of the hypothermia, hemofiltration, and the potential sequestration of allopurinol in the circuit. The reduced CL of oxypurinol after CPB is likely attributable to impaired kidney function.
© 2024. The Author(s).
Conflict of interest statement
Wan-Yu Chu, Maaike Nijman, Raymond Stegeman, Johannes M. P. J. Breur, Nicolaas J.G. Jansen, Joppe Nijman, Kim van Loon, Erik Koomen, Karel Allegaert, Manon J.N.L. Benders, Thomas P.C. Dorlo, and Alwin D.R. Huitema have no conflicts of interest to declare that may be relevant to the contents of this article.
Figures




References
-
- Stegeman R, Feldmann M, Claessens NHP, Jansen NJG, Breur JMPJ, de Vries LS, et al. A uniform description of perioperative brain MRI findings in infants with severe congenital heart disease: results of a European Collaboration. AJNR Am J Neuroradiol. 2021;42:2034–9. 10.3174/ajnr.A7328 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
