

Monitoring response to neoadjuvant chemotherapy in triple negative breast cancer using circulating tumor DNA
- PMID: 39148033
- PMCID: PMC11328413
- DOI: 10.1186/s12885-024-12689-6
Monitoring response to neoadjuvant chemotherapy in triple negative breast cancer using circulating tumor DNA
Abstract
Background: Triple negative breast cancer (TNBC) is an aggressive subtype with poor prognosis. We aimed to determine whether circulating tumor DNA (ctDNA) and circulating tumor cell (CTC) could predict response and long-term outcomes to neoadjuvant chemotherapy (NAC).
Methods: Patients with TNBC were enrolled between 2017-2021 at The University of Texas MD Anderson Cancer Center (Houston, TX). Serial plasma samples were collected at four timepoints: pre-NAC (baseline), 12-weeks after NAC (mid-NAC), after NAC/prior to surgery (post-NAC), and one-year after surgery. ctDNA was quantified using a tumor-informed ctDNA assay (SignateraTM, Natera, Inc.) and CTC enumeration using CellSearch. Wilcoxon and Fisher's exact tests were used for comparisons between groups and Kaplan-Meier analysis used for survival outcomes.
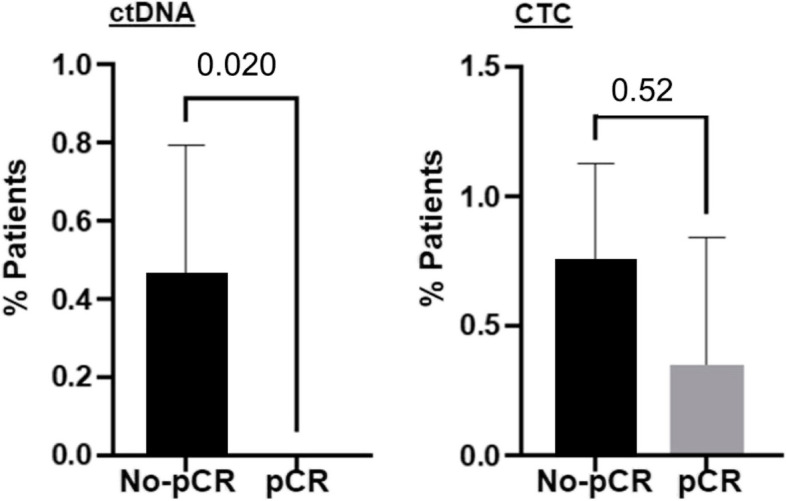
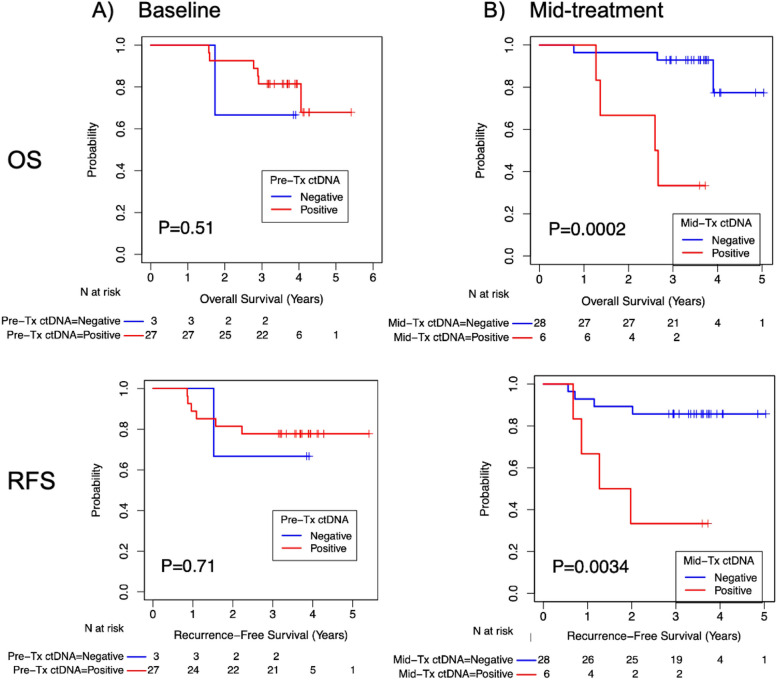
Results: In total, 37 patients were enrolled. The mean age was 50 and majority of patients had invasive ductal carcinoma (34, 91.9%) with clinical T2, (25, 67.6%) node-negative disease (21, 56.8%). Baseline ctDNA was detected in 90% (27/30) of patients, of whom 70.4% (19/27) achieved ctDNA clearance by mid-NAC. ctDNA clearance at mid-NAC was significantly associated with pathologic complete response (p = 0.02), whereas CTC clearance was not (p = 0.52). There were no differences in overall survival (OS) and recurrence-free survival (RFS) with positive baseline ctDNA and CTC. However, positive ctDNA at mid-NAC was significantly associated with worse OS and RFS (p = 0.0002 and p = 0.0034, respectively).
Conclusions: Early clearance of ctDNA served as a predictive and prognostic marker in TNBC. Personalized ctDNA monitoring during NAC may help predict response and guide treatment.
Keywords: CTC; Liquid biopsy; Liquid biopsy in neoadjuvant setting; Triple negative breast cancer; ctDNA.
© 2024. The Author(s).
Conflict of interest statement
E.K., E.S., H.S., A.R., and M.C.L. are employees of Natera, Inc. and have stock/option to hold stock in the company. Additional COIs for M.C.L: Grants/Contracts: Funding to Institution (Mayo) from: Eisai, Exact Sciences, Genentech, Genomic Health, GRAIL, Menarini Silicon Biosystems, Merck, Novartis, Seattle Genetics, Tesaro; Travel Support Reimbursement from AstraZeneca, Genomic Health, Ionis; Ad hoc advisory board meetings. All funds to Mayo Clinic. No personal compensation from: AstraZeneca, Celgene, Roche/Genentech, Genomic Health, GRAIL, Ionis, Merck, Pfizer, Seattle Genetics, Syndax.
Figures



References
-
- Ismail-Khan R, Bui MM. A Review of Triple-Negative Breast Cancer. Cancer Control [Internet]. SAGE Publications Inc; 2010;17:173–6. Available from: 10.1177/107327481001700305 - PubMed
-
- Han HS, Vikas P, Costa RLB, Jahan N, Taye A, Stringer-Reasor EM. Early-Stage Triple-Negative Breast Cancer Journey: Beginning, End, and Everything in Between. American Society of Clinical Oncology Educational Book [Internet]. Wolters Kluwer; 2023;e390464. Available from: 10.1200/EDBK_390464 - PubMed
-
- Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, et al. Triple-Negative Breast Cancer: Clinical Features and Patterns of Recurrence. Clinical Cancer Research [Internet]. 2007;13:4429–34. Available from: 10.1158/1078-0432.CCR-06-3045 - PubMed
-
- Foulkes WD, Smith IE, Reis-Filho JS. Triple-Negative Breast Cancer. New England Journal of Medicine [Internet]. Massachusetts Medical Society; 2010;363:1938–48. Available from: 10.1056/NEJMra1001389 - PubMed
-
- Liedtke C, Mazouni C, Hess KR, André F, Tordai A, Mejia JA, et al. Response to Neoadjuvant Therapy and Long-Term Survival in Patients With Triple-Negative Breast Cancer. Journal of Clinical Oncology [Internet]. Wolters Kluwer; 2023;41:1809–15. Available from: 10.1200/JCO.22.02572 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
