

This is a preprint.
Neoadjuvant cabozantinib restores CD8+ T cells in patients with locally advanced non-metastatic clear cell renal cell carcinoma: a phase 2 trial
- PMID: 39149474
- PMCID: PMC11326393
- DOI: 10.21203/rs.3.rs-4849400/v1
Neoadjuvant cabozantinib restores CD8+ T cells in patients with locally advanced non-metastatic clear cell renal cell carcinoma: a phase 2 trial
Update in
-
Neoadjuvant cabozantinib for locally advanced nonmetastatic clear cell renal cell carcinoma: a phase 2 trial.Nat Cancer. 2025 Mar;6(3):432-444. doi: 10.1038/s43018-025-00922-5. Epub 2025 Feb 27. Nat Cancer. 2025. PMID: 40016487 Clinical Trial.
Abstract
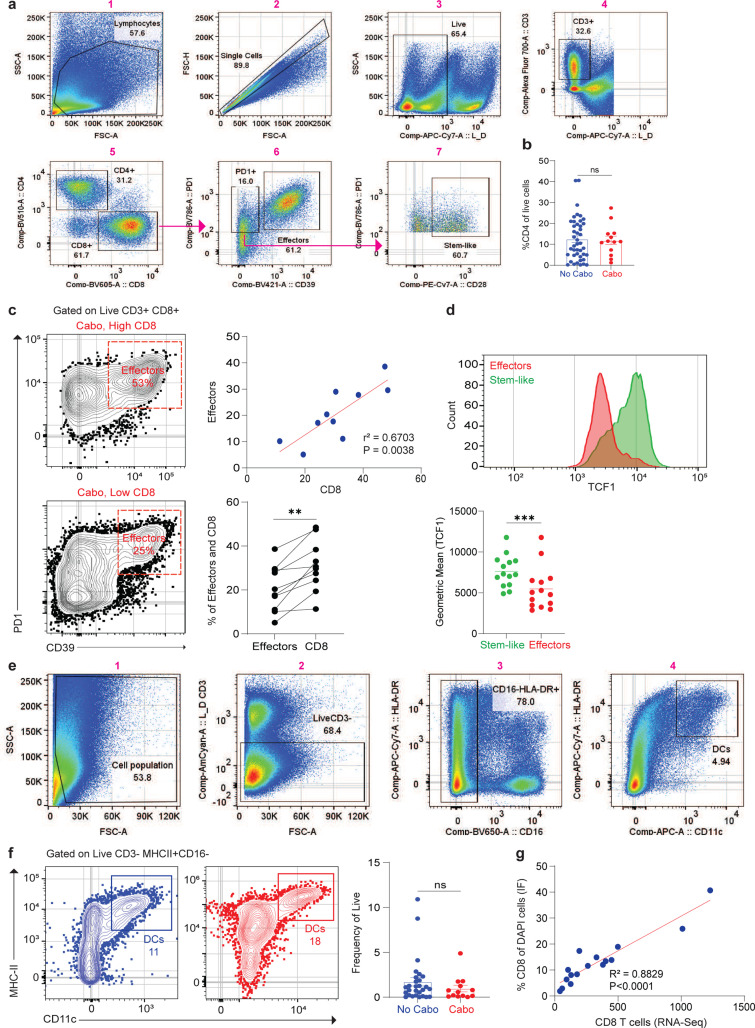
Cabozantinib is an oral multikinase inhibitor approved for treatment in metastatic renal cell carcinoma (RCC). We hypothesized that neoadjuvant cabozantinib could downstage localized tumors, facilitating partial nephrectomy, and facilitating surgery in patients with locally advanced tumors that would require significant adjacent organ resection. We, therefore, conducted a phase 2, single-arm trial of cabozantinib treatment for 12 weeks in 17 patients with locally advanced biopsy-proven non-metastatic clear cell RCC before surgical resection. Six patients (35%) experienced a partial response, and 11 patients (65%) had stable disease. We identified that plasma cell-free DNA (cfDNA), VEGF, c-MET, Gas6, and AXL were significantly increased while VEGFR2 decreased during cabozantinib treatments. There was a trend towards CD8+ T cells becoming activated in the blood, expressing the proliferation marker Ki67 and activation markers HLA-DR and CD38. Cabozantinib treatment depleted myeloid populations acutely. Importantly, immune niches made up of the stem-like CD8+ T cells and antigen presenting cells were increased in every patient. These data suggest that cabozantinib treatment was clinically active and safe in the neoadjuvant setting in patients with locally advanced non-metastatic clear cell RCC and activated the anti-tumor CD8+ T cell response. The trial is registered at ClinicalTrials.gov under registration no. NCT04022343.
Conflict of interest statement
Completing interests M.A.B. has acted as a paid consultant for and/or as a member of the advisory boards of Exelixis, Bayer, BMS, Eisai, Pfizer, AstraZeneca, Janssen, Calithera Biosciences, Genomic Health, Nektar, EMD Serono, SeaGen, and Sanofi and has received grants to his institution from Merck, Xencor, Bayer, Bristol-Myers Squibb, Genentech/Roche, SeaGen, Incyte, Nektar, AstraZeneca, Tricon Pharmaceuticals, Exelixis, Nikang, Loxo Oncology, Ambrx, Regeneron, Acrivon Therapeutics, Amgen, Genome & Company, AAA, Peloton Therapeutics, and Pfizer for work performed as outside of the current study. The other authors declare no competing interests.
Figures









References
Publication types
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
