

This is a preprint.
Optimizing Transcutaneous Spinal Stimulation: Excitability of Evoked Spinal Reflexes is Dependent on Electrode Montage
- PMID: 39149487
- PMCID: PMC11326363
- DOI: 10.21203/rs.3.rs-4719031/v1
Optimizing Transcutaneous Spinal Stimulation: Excitability of Evoked Spinal Reflexes is Dependent on Electrode Montage
Update in
-
Optimizing transcutaneous spinal stimulation: excitability of evoked spinal reflexes is dependent on electrode montage.J Neuroeng Rehabil. 2025 Jan 6;22(1):2. doi: 10.1186/s12984-024-01524-5. J Neuroeng Rehabil. 2025. PMID: 39762915 Free PMC article. Clinical Trial.
Abstract
Background: There is growing interest in use of transcutaneous spinal stimulation (TSS) for people with neurologic conditions both to augment volitional control (by facilitating motoneuron excitability), and to decrease spasticity (by activating inhibitory networks). Various electrode montages are used during TSS, with little understanding of how electrode position influences spinal circuit activation. We sought to identify the thoracolumbar electrode montage associated with the most robust activation of spinal circuits by comparing posterior root-muscle reflexes (PRM reflexes) elicited by 6 montages. Additionally, we assessed tolerability of the stimulation during PRM reflex testing.
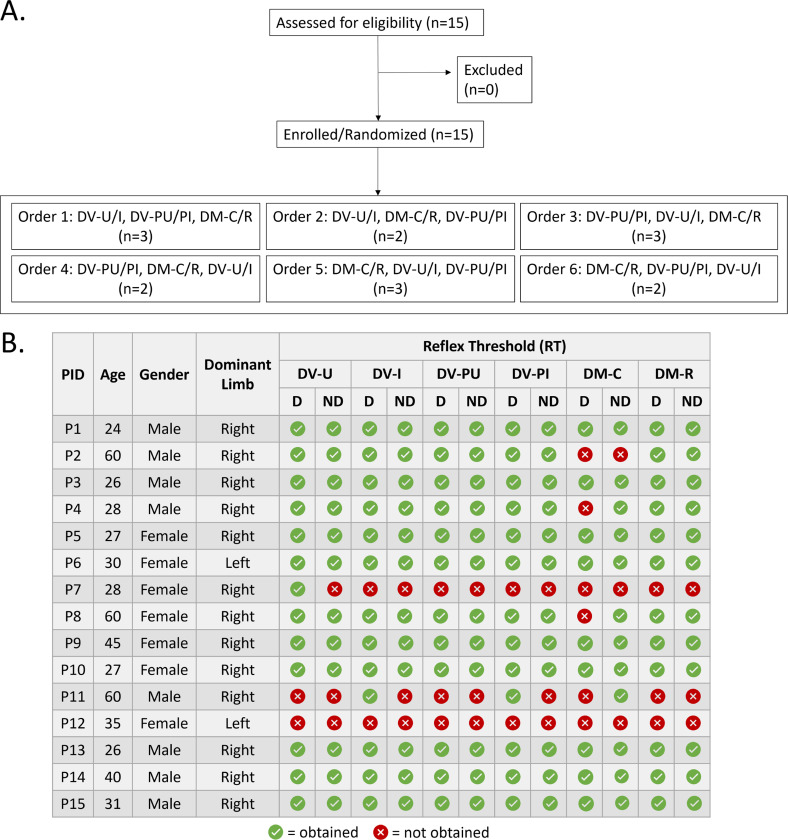
Methods: Fifteen adults with intact neurological systems participated in this randomized crossover study. PRM reflexes were evoked transcutaneously using electrode montages with dorsal-ventral (DV) or dorsal-midline (DM) current flow. DV montages included: [1] cathode over T11/T12, anodes over iliac crests (DV-I), [2] cathode over T11/T12, anodes over umbilicus (DV-U), [3] dual paraspinal cathodes at T11/12, anodes over iliac crests (DV-PI), and [4] dual paraspinal cathodes at T11/12, anodes over umbilicus (DV-PU). DM montages included: [5] cathode over T11/12, anode 5cm caudal (DM-C), and [6] cathode over T11/12, anode 5cm rostral (DM-R). PRM reflex recruitment curves were obtained in the soleus muscle of both lower extremities.
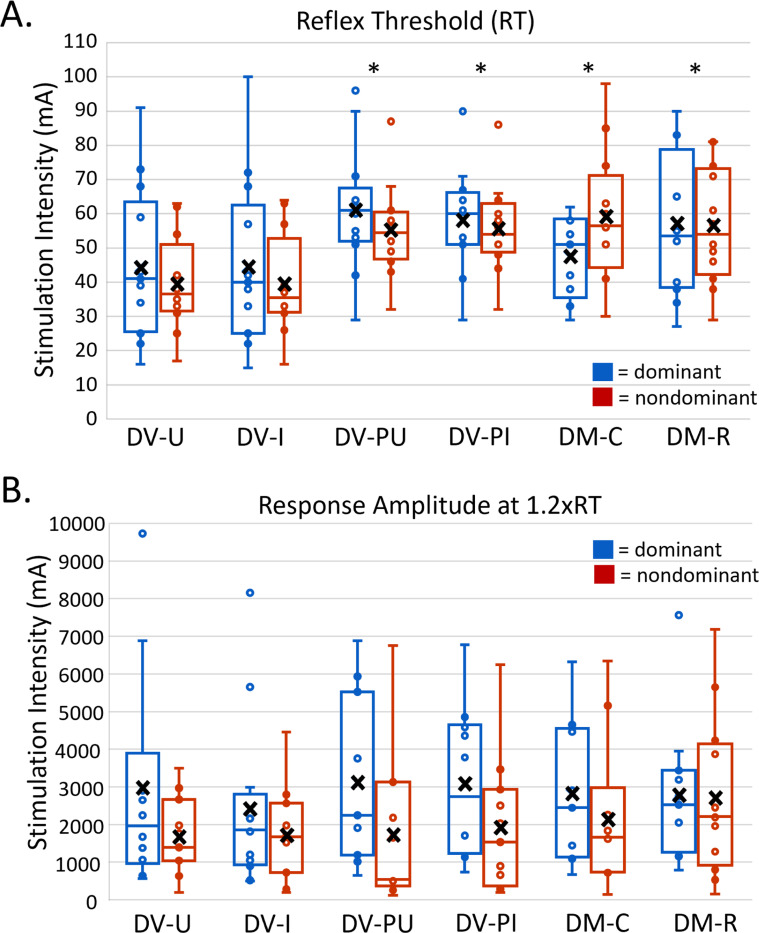
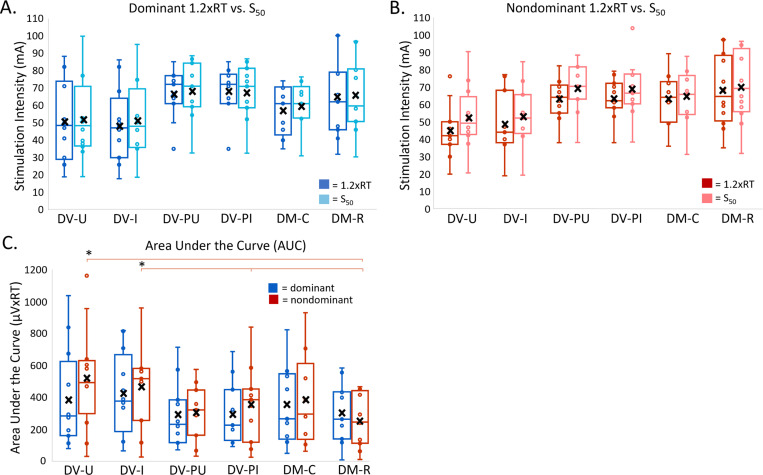
Results: DV-U and DV-I montages elicited bilateral reflexes with lower reflex thresholds and larger recruitment curve area than other montages. There were no differences in response amplitude at 120% of RT(1.2xRT) or tolerability among montages.
Conclusions: Differences in spinal circuit recruitment are reflected in the response amplitude of the PRM reflexes. DV-I and DV-U montages were associated with lower reflex thresholds, indicating that motor responses can be evoked with lower stimulation intensity. DV-I and DV-U montages therefore have the potential for lower and more tolerable interventional stimulation intensities. Our findings optimize electrode placement for interventional TSS and PRM reflex assessments.
Keywords: Electrodes; Neuromodulation; Spinal Excitability; Transcutaneous Spinal Stimulation.
Conflict of interest statement
Competing Interests: Author ECF-F serves as a consultant to the medical device company ONWARD Inc.
Figures


Similar articles
-
Optimizing transcutaneous spinal stimulation: excitability of evoked spinal reflexes is dependent on electrode montage.J Neuroeng Rehabil. 2025 Jan 6;22(1):2. doi: 10.1186/s12984-024-01524-5. J Neuroeng Rehabil. 2025. PMID: 39762915 Free PMC article. Clinical Trial.
-
Bipolar transcutaneous spinal stimulation evokes short-latency reflex responses in human lower limbs alike standard unipolar electrode configuration.J Neurophysiol. 2020 Oct 1;124(4):1072-1082. doi: 10.1152/jn.00433.2020. Epub 2020 Aug 26. J Neurophysiol. 2020. PMID: 32845202
-
Recovery cycles of posterior root-muscle reflexes evoked by transcutaneous spinal cord stimulation and of the H reflex in individuals with intact and injured spinal cord.PLoS One. 2019 Dec 26;14(12):e0227057. doi: 10.1371/journal.pone.0227057. eCollection 2019. PLoS One. 2019. PMID: 31877192 Free PMC article.
-
Distinguishing reflex from non-reflex responses elicited by transcutaneous spinal stimulation targeting the lumbosacral cord in healthy individuals.Exp Brain Res. 2024 Apr;242(4):959-970. doi: 10.1007/s00221-024-06790-2. Epub 2024 Feb 28. Exp Brain Res. 2024. PMID: 38416179 Free PMC article.
-
Modulations in neural pathways excitability post transcutaneous spinal cord stimulation among individuals with spinal cord injury: a systematic review.Front Neurosci. 2024 Mar 25;18:1372222. doi: 10.3389/fnins.2024.1372222. eCollection 2024. Front Neurosci. 2024. PMID: 38591069 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
