

Demographic and Metabolic Risk Factors Associated with Development of Diabetic Macular Edema among Persons with Diabetes Mellitus
- PMID: 39149711
- PMCID: PMC11324816
- DOI: 10.1016/j.xops.2024.100557
Demographic and Metabolic Risk Factors Associated with Development of Diabetic Macular Edema among Persons with Diabetes Mellitus
Abstract
Purpose: Diabetic macular edema (DME), a leading cause of visual impairment, can occur regardless of diabetic retinopathy (DR) stage. Poor metabolic control is hypothesized to contribute to DME development, although large-scale studies have yet to identify such an association. This study aims to determine whether measurable markers of dysmetabolism are associated with DME development in persons with diabetes.
Design: Retrospective cohort study.
Participants: Using data from the Sight Outcomes Research Collaborative (SOURCE) repository, patients with diabetes mellitus and no preexisting DME were identified and followed over time to see what factors associated with DME development.
Methods: Cox proportional hazard modeling was used to assess the relationship between demographic variables, diabetes type, smoking history, baseline DR status, blood pressure (BP), lipid profile, body mass index (BMI), hemoglobin A1C (HbA1C), and new onset of DME.
Main outcome measures: Adjusted hazard ratio (HR) of developing DME with 95% confidence intervals (CIs).
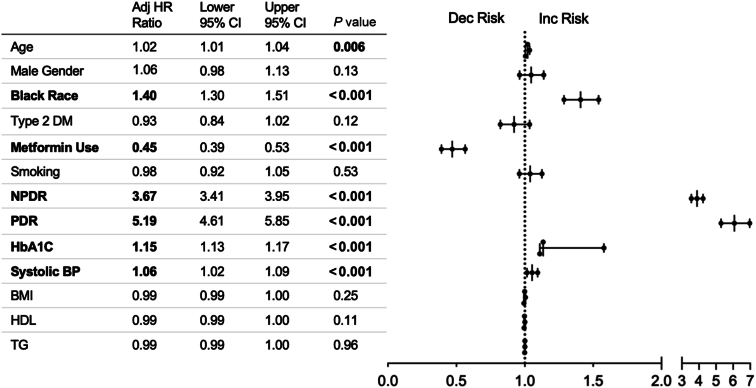
Results: Of 47 509 eligible patients from 10 SOURCE sites (mean age 63 ± 12 years, 58% female sex, 48% White race), 3633 (7.6%) developed DME in the study period. The mean ± standard deviation time to DME was 875 ± 684 days (∼2.4 years) with those with baseline nonproliferative DR (HR 3.67, 95% CI: 3.41-3.95) and proliferative DR (HR 5.19, 95% CI: 4.61-5.85) more likely to develop DME. There was no difference in DME risk between type 1 and type 2 patients; however, Black race was associated with a 40% increase in DME risk (HR 1.40, 95% CI: 1.30-1.51). Every 1 unit increase in HbA1C had a 15% increased risk of DME (HR 1.15, 95% CI: 1.13-1.17), and each 10 mmHg increase in systolic BP was associated with a 6% increased DME risk (HR 1.06, 95% CI: 1.02-1.09). No association was identified between DME development and BMI, triglyceride levels, or high-density lipoprotein levels.
Conclusions: These findings suggest that in patients with diabetes modifiable risk factors such as elevated HbA1C and BP confer a higher risk of DME development; however, other modifiable systemic markers of dysmetabolism such as obesity and dyslipidemia did not. Further work is needed to identify the underlying contributions of race in DME.
Financial disclosures: Proprietary or commercial disclosure may be found in the Footnotes and Disclosures at the end of this article.
Keywords: Black race; Blood pressure; Diabetic macular edema; Diabetic retinopathy; Metabolic syndrome.
© 2024 by the American Academy of Ophthalmology.
Figures


References
-
- Das A., McGuire P.G., Rangasamy S. Diabetic macular edema: pathophysiology and novel therapeutic targets. Ophthalmology. 2015;122:1375–1394. - PubMed
-
- Klein R., Klein B.E., Moss S.E., et al. The Wisconsin epidemiologic study of diabetic retinopathy. IV. Diabetic macular edema. Ophthalmology. 1984;91:1464–1474. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
