

Nephrocalcinosis and kidney function in children and adults with X-linked hypophosphatemia: baseline results from a large longitudinal study
- PMID: 39151033
- PMCID: PMC11425691
- DOI: 10.1093/jbmr/zjae127
Nephrocalcinosis and kidney function in children and adults with X-linked hypophosphatemia: baseline results from a large longitudinal study
Abstract
Background: In patients with X-linked hypophosphatemia (XLH), conventional therapy with oral phosphate salts and active vitamin D has been associated with nephrocalcinosis. However, the nature of the relationships among XLH, its treatment, nephrocalcinosis, and kidney function remain poorly understood.
Methods: Renal ultrasounds were performed and glomerular filtration rates were estimated (eGFR) at baseline in burosumab-naïve patients with XLH who participated in burosumab clinical trials (NCT02181764, NCT02526160, NCT02537431, NCT02163577, NCT02750618, NCT02915705) or enrolled in the XLH Disease Monitoring Program (XLH-DMP; NCT03651505). In this cross-sectional analysis, patient, disease, and treatment characteristics were described among patients with and without nephrocalcinosis.
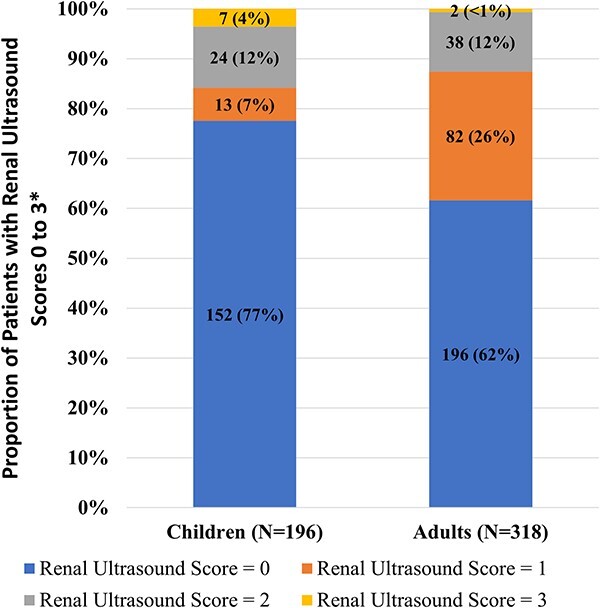
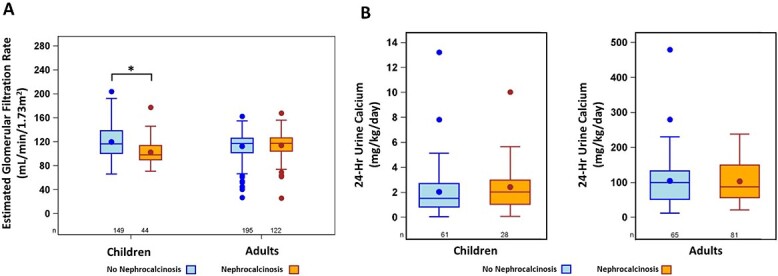
Results: The analysis included 196 children (mean [SD] age 7.6 [4.0] yr) and 318 adults (40.3 [13.1] yr). Mean (SD) height z-score was -1.9 (1.2) for children and -2.3 (1.7) for adults. Nearly all children (97%) and adults (94%) had previously received conventional therapy. Nephrocalcinosis was detected in 22% of children and 38% of adults. In children, reduced eGFR <90 mL/min/1.73 m2 was more prevalent in those with nephrocalcinosis (25%) than in those without (11%), a finding that was not observed in adults. Children with nephrocalcinosis had lower mean values of TmP/GFR (p<.05), serum 1,25(OH)2D (p<.05), and eGFR (p<.001) and higher mean serum calcium concentrations (p<.05) than did those without nephrocalcinosis. Adults with nephrocalcinosis had lower mean serum phosphorus (p<.01) and 1,25(OH)2D (p<.05) concentrations than those without. Exploratory logistic regression analyses revealed no significant associations between the presence of nephrocalcinosis and other described patient or disease characteristics.
Conclusions: Nephrocalcinosis was observed in nearly one-quarter of children and more than one-third of adults with XLH. Further study is needed to better understand the predictors and long-term consequences of nephrocalcinosis, with surveillance for nephrocalcinosis remaining important in the management of XLH.
Keywords: X-linked hypophosphatemia; active vitamin D; hyperparathyroidism; nephrocalcinosis; phosphate; renal function.
Plain language summary
Conventionally, patients with X-linked hypophosphatemia (XLH) were treated with phosphate and vitamin D taken by mouth. However, this therapy might lead to a buildup of calcium in the kidney, called nephrocalcinosis. Here, we tried to better understand how XLH, conventional therapy, nephrocalcinosis, and kidney function are related. Nephrocalcinosis was detected with kidney ultrasounds. Kidney function, called the estimated glomerular filtration rate (eGFR), was determined using blood levels of creatinine. Patients had been part of burosumab clinical trials or part of the XLH Disease Monitoring Program. Data were collected from patients before they received burosumab. The study included 196 children and 318 adults. Almost all children and adults had received conventional therapy. 22% of children and 38% of adults had nephrocalcinosis. Some lab values were different among patients with vs without nephrocalcinosis. Children with nephrocalcinosis had significantly greater loss of phosphate by the kidneys, lower blood levels of the active form of vitamin D (1,25(OH)2D), lower eGFR, and higher blood levels of calcium than those without nephrocalcinosis. Adults with nephrocalcinosis had significantly lower blood levels of phosphorus and 1,25(OH)2D concentrations than those without. It remains important to monitor patients with XLH for nephrocalcinosis. Further study is needed to better understand nephrocalcinosis.
© The Author(s) 2024. Published by Oxford University Press on behalf of the American Society for Bone and Mineral Research.
Conflict of interest statement
A.C., C.W., M.S.R., P.K.T., and C.B. are, or were, employees and stockholders of Ultragenyx Pharmaceutical Inc. at the time this study was conducted. All other authors are PIs in the XLH-DMP. A.A.P. has been a consultant to, and served as an investigator in clinical trials with Ultragenyx Pharmaceutical Inc. S.J. is a consultant, and on a scientific advisory board for Kyowa Kirin International and an investigator, consultant and on a scientific advisory board for Ultragenyx Pharmaceutical Inc. K.D.R. is a clinical trial investigator and advisor for Ultragenyx Pharmaceutical Inc. A.I.M.M. is a speaker for Ultragenyx Pharmaceutical Inc. E.A.I. has research grants to his institution from Ultragenyx and Kyowa Kirin and has served on advisory boards for these companies. S.I. has received research grants paid to his institution from Alexion, Amgen, Amolyt, AstraZeneca Rare Disease, Calcilytix, Radius, Takeda, and Ultragenyx, and has served on an advisory board and/or consultant for Amgen, Bone Health & Osteoporosis Foundation, Extend Biosciences, Radius, and Soft Bones, Inc. L.W. declares participating in clinical trials with Ultragenyx, with funds to Dr Ward’s institution, and consultancy to, and unrestricted educational grants from, Utragenyx and Kyowa Kirin, with funds to Dr Ward’s institution.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
